
Suprascapular Nerve Palsy
Where is it?
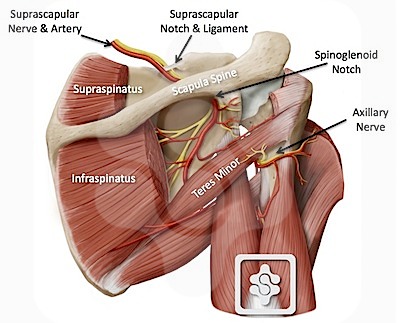
The brachial plexus is a large bundle of nerves which innervates the arm and upper portions of the chest. Its origins are in five nerves coming from five different parts of an area known as the cervical spine (from C5 to T1). The first two nerves (C5 and C6) combine to form what is known as the superior trunk. It is from this structure that the suprascapular nerve originates. From the trunk it passes inferiorly (downwards) under the trapezius muscle towards the superior (top) edge of the scapula, otherwise known as the shoulder blade. After passing through the scapular notch the nerve takes a turn obliquely and laterally (diagonally outwards) towards the first muscle that it supplies, the supraspinatus. Here, the nerve splits, with one thick branch staying with the supraspinatus and one heading towards the other muscle it supplies, the infraspinatus.
What is it?
Palsy is a word that is derived from paralysis and can mean anything from a weakness to a complete paralysis. It can result from any sort of damage to the nerve. Three of the most likely cause's are:
- Entrapment of the nerve within the suprascapular notch or the spinoglenoid notch. The cause of this may be:
- Paralabral ganglion cyst - pressing on the nerve
- Thickening and/or bony ossification (bony change) of the overlying ligament (Superior Transverse Scapula Ligament - STSL).
- A major or repetitive trauma . Major trauma can result from a fractured scapula, a tear of the rotator cuff or shoulder arthrodesis. These can all cause a compression of the nerve. Repetitive trauma is most likely the cause of repetitive overhead loading as seen mainly in sports such as tennis, weight lifting, boxing or baseball. It can also be seen in certain professions such as painters and decorators.
- Neuralgic amyotrophy : a relatively uncommon condition, it is characterised by an acute onset of shoulder pain and weakness. The condition is not very well understood but is thought that it may be due to an infection with certain viruses such as CMV, or may follow the administration of certain vaccines.
When there is any sort of disruption within the suprascapular nerve, the muscles it supplies (supraspinatus and infraspinatus) lose their innervation, which causes the signs and symptoms seen with a suprascapular nerve palsy.
Signs, Symptoms and Diagnosis
The muscles supplied by the suprascapular nerve are the supraspinatus and infraspinatus . These muscles are part of the rotator cuff and help with movements of the arm at the shoulder joint.
If these become weakened or wasted due to a lack of innervations then those movements will suffer as a result.
If the supraspinatus is affected then abduction at the shoulder joint may be affected. This is the movement of bringing your arms up from your sides to clap above your head.
If the infraspinatus is affected then external rotation may be affected. This movement is similar to that used when reaching backwards to put on a seatbelt in a car.
Wasting of this muscles is usuually visible when looking at the shoulder from behind.
Pain is variable. Sometimes impingement pain is present and sometimes there is a general ache around the shoulder and shoulder blade after activities. In neuralgic amyotrophy severe pain may be present in the early stages. Pain may radiate to the back, neck or upper part of the chest.

Diagnosis can usually be confirmed with a special study called electromyography (EMG) which would show denervation of the involved muscles. MRI scans are helpful to diagnose a ganglion cyst and confrim the pattern of muscle wasting. However, the diagnosis is made on a purely clinical ground, i.e. just on the history and examination.
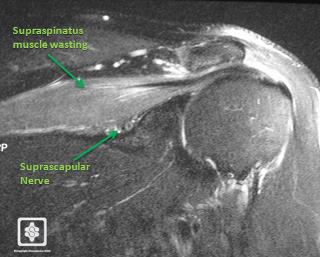
MRI Scan showing wasting of the supraspinatus muscle, with fatty infiltration (the supraspinatus muscle looks whiter than the other muscles on this MRI sequence). You can also see the suprascapular nerve under the muscle.
Treatment
Treatment is usually involves physiotherapy, with specific reactivation exercises and a scapula control regimen. Avoidance of worsening activities should be observed to give the nerve time to recover without further aggravation or stretching.
Occasionally surgery may be needed, especially if the cause of the problem is entrapment or compression.
It is usually done by open surgery. We prefer to do this by arthroscopy (keyhole surgery) , however this is a very new technique and only available in few centres around the world.
For details of the Endoscopic Procedure see below .
For details of the Open Procedure click here .
Endoscopic Suprascapular Nerve Decompression
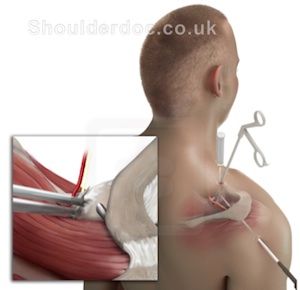
Advances in keyhole surgery (arthroscopy/endoscopy) of the shoulder have made decompression of the suprascapular nerve via this route possible. Since the nerve is deeply buried under the large muscles of the shoulder endoscopic techniques are well suited for decompressing the nerve.
The nerve is decompressed via three small keyholes. The ligament over the nerve is cut allowing more space for the nerve:
Below is a surgical video of the procedure:
GENERAL GUIDELINES
PAIN
A nerve block is not used during the operation as it can interfere with the nerve. You will be given painkillers whilst in hospital. These can be continued after you are discharged home. Ice packs or a commercial Cold compression wrap may also help reduce pain. Wrap frozen peas or crushed ice in a damp, cold cloth and place on the shoulder for up to 15 minutes. In order to maintain a dry wound cover the dressing / wound with some cling film before applying the ice pack.
Click Here for more information
THE WOUND
This is a keyhole operation usually done through three or four 5mm puncture wounds. There will be no stitches only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 5 to 7 days.

WEARING A SLING
You will return from theatre wearing a sling and/or Cold compression wrap. This is for comfort only and should be discarded as soon as possible (usually within the first 2 to 4 days). Some people find it helpful to continue to wear the sling at night for a little longer if the shoulder feels tender.
DRIVING
You may begin driving one week after your operation or when you feel comfortable.
RETURNING TO WORK
This will depend on your occupation. If you are in a sedentary job you may return as soon as you feel able usually after one week.
If your job involves heavy lifting or using your arm above shoulder height you may require a longer period of absence.
LEISURE ACTIVITIES
You should avoid sustained, repetitive overhead activities for three months. With regard to swimming you may begin breaststroke as soon as you are comfortable but you should wait three months before resuming front crawl. Golf can begin at six weeks. For guidance on DIY and racquet sports you should speak with your physiotherapist.
FOLLOW UP APPOINTMENT
A follow up appointment will be made for approximately three weeks after your operation. The amount of physiotherapy will depend on your individual needs.
PROGRESS
This is variable. However experience shows us that by 3 weeks movement below shoulder height becomes more comfortable. By this stage you should have almost full range of movement although there will probably be discomfort when moving the arm above the head and when lying directly on your shoulder.
At three months after your surgery your symptoms should be approximately 80% better. It can take 6 to 9 months to fully recover and you will continue to improve for up to a 18 months following the procedure.
PHYSIOTHERAPY
Physiotherapy is essential after the operation, to encourage good movement, help with pain management and rehabilitate the muscles back to normal function. You will need to see a therapist within 2 weeks of the surgery. This should be arranged in advance of the surgery. I list of therapists with an interest in shoulders can be found here.
