
Quadrilateral Space Syndrome
Lennard Funk
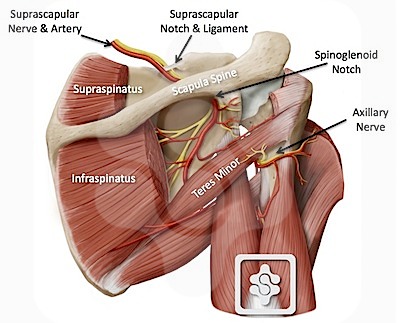
The quadrilateral space is located posterior and inferior to the glenohumeral joint and contains the axillary nerve and posterior humeral circumflex artery. The space is bounded superiorly by the teres minor muscle, inferiorly by the teres major muscle, medially by the long head of the triceps, and laterally by the humeral shaft.
Quadrilateral space syndrome (QSS) is compression of the axillary nerve and posterior humeral circumflex artery as they pass through this space.
This is a vary rare condition, but should be suspected in athletes with the symptoms below.
Aetiology:
The typical causes of QSS are:
- Fibrous bands in the quadrilateral space, tightening in abduction and external rotation.
- Paralabral cysts, associated with inferior labral tears is the commonest cause we have found, especially in contact athletes.
- Very rarely: tumours and haematomas
Clinical Presentation:
QSS typically occurs in in young athletic adults in the age range of 25 to 35 years without a history of significant trauma.
The pain is characterized clinically by a dull intermittent ache localized in the posterior and lateral shoulder. These symptoms are exacerbated by active and resisted abduction and external rotation of the humerus. Point tenderness is often present overlying the quadrilateral space posteriorly at the insertion site of the teres minor. Atrophy or weakness of the teres minor and deltoid muscle may also be noted.Paresthesias mayy occur in the cutaneous sensory distribution of the axillary nerve, overlying the deltoid muscle in the lateral shoulder and upper posterior arm.
The diagnosis of QSS can be difficult and many patients with this condition are often diagnosed and treated for other conditions before the diagnosis is finally made. This can complicate the clinical picture. Often patients will have been misdiagnosed as impingement and had subacromial decompressions or other interventions.
Investigations:
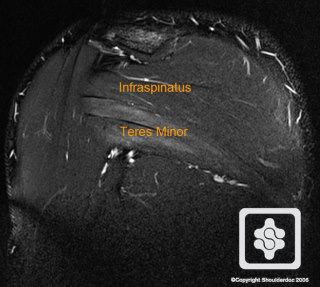
MRI Scan - this will demonstrate the atrophy of teres minor (and rarely deltoid) and show any large paralabral cysts, tumours or haematomas.
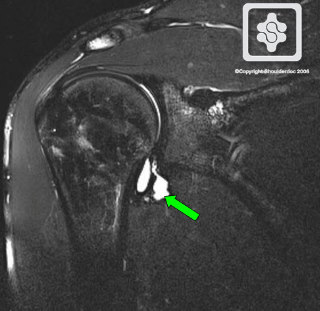
MR Arthrogram - will demonstrate all the above, plus any associated labral lesions (Our preferred scan)
MR Arthrogram showing a typical inferior paralabral cyst associated with a labral tear, causing QSS
MRI Scan showing atrophy of Teres Minor
Treatment:
For minor symptoms, little weakness and no significant mass lesion on MR scanning rehabilitation and functional strengthening can result in improvements over a few months.
For significant weakness and functional disability surgical decompression is indicated. Parlabral cysts can be approached arthroscopically and the associated labral tear repaired. Other large mass lesions require open surgical excision.
Outcomes:
Successful appropriate treatment should result in full recovery. Case Studies in the literature report full recovery within 3-6 months.
REFERENCES
- McAdams TR, Dillingham DF. Surgical Decompression of the Quadrilateral Space in Overhead Athletes. Am J Sports Med. 36:538-32. 2008.
- Cahill BR, Palmer RE. Quadrilateral space syndrome. J Hand Surg
Am. 1983;8:65-69. - Chautems RC, Glauser T, Waeber-Fey MC, Rostan O, Barraud GE. Quadrilateral space syndrome: case report and review of the literature. Ann Vasc Surg. 2000;14(6):673-676.
- Cormier PJ, Matalon TA, Wolin PM. Quadrilateral space syndrome: a rare cause of shoulder pain. Radiology. 1988;167:797-798.
- Cothran RL, Helms C. Quadrilateral space syndrome: incidence of imaging findings in a population referred for MRI of the shoulder. AJR Am J Roentgenol. 2005;184:989-992.
- Francel TJ, Dellon AL, Campbell JN. Quadrilateral space syndrome: diagnosis and operative decompression technique. Plast Reconstr Surg. 1991;87(5):911-916.
- Hoskins WT, Pollard HP, McDonald AJ. Quadrilateral space Syndrome: a case study and review of the literature. Br J Sports Med. 2005;39(9):e9.
- Ishima T, Usui M, Satoh E, Sakahashi H, Okamura K. Quadrilateral space syndrome caused by a ganglion. J Shoulder Elbow Surg. 1998;7(1):80-82.
- Lester B, Jeong GK, Weiland AJ, Wickiewicz TL. Quadrilateral space syndrome: diagnosis, pathology, and treatment. Am J Orthop. 1999;12:718-722.
- Okino S, Miyaji H, Matoba M. The quadrilateral space syndrome. Neuroradiology. 1995;37(4):311-312.
- Redler MR, Ruland LJ, McCue FC. Quadrilateral space syndrome in a throwing athlete. Am J Sports Med. 1986;14(8):511-513.
- Robinson P, White LM, Lax M, Salonen D, Bell RS. Quadrilateral space syndrome caused by a glenoid labral cyst. AJR Am J Roentgenol. 2000;175:1103-1105.
- Safran MR. Nerve injury about the shoulder in athletes, part I: suprascapular and axillary nerve. Am J Sports Med. 2004;32:803-819.
- Sanders TG, Tirman PF. Paralabral cyst: an unusual cause of quadrilateral space syndrome. Arthroscopy. 1999;15(6):632-637
