
Pec Major Transfer for Serratus Palsy
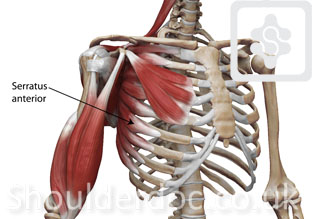
The serratus anterior is a group of muscles that attach the front of the shoulder blade (scapula) to the ribcage. The muscle stabilises the scapula during overhead movements and rotates is forward to allow forward elevation of the arm.
Winging of the scapula due to a serratus anterior muscle weakness is uncommon, but it does affect young and active people. It can therefore be very debilitating. EMG studies will identify the lesion of the long thoracic nerve or muscle and the recovery. Most recover spontaneously over an 18 month period without surgery, but some remain permanent lesions. The winging can cause discomfort and weakness of the shoulder complex with any manual activities, particularly heavy repetitive overhead work.
In isolated serratus anterior winging with no improvement pec major muscle transfer may be an option to correct the winging and improve the discomfort and strength.
OPERATIVE TECHNIQUE:
The operation is performed under general anaesthesia with an interscalene block.
An incision is made at the front of the shoulder to detach the pec major from the humerus. Usually one half to two thirds of the pec major tendon is detached and mobilised.
A second incision is made at the back of the shoulder, over the scapula, where the scapula is prepared for attachment of the transferred tendon. The pec major tendon is then 'tunnelled' from the front of the body to the incision at the back, going under the skin. The tendon is then attached with the appropriate tension to the border of the scapula. It is essential for the surgeon to get the tension of the repair right. This depends on skill, training and experience. Occasionally some additional tissue augmentation may be required. This may be tendon (tensor fascia lata) from the thigh area, or allograft tissue or a synthetic collagen mesh. The surgeon will discuss this with you before the surgery. The transferred tendon is then fixed to the bone with multiple strong suture-anchors.
Transferred Pec Major tendon to the scapula:
![]()
COMPLICATIONS:
Complications include infection, stiffness and failure of the transfer. The incidence of these is less than 1%.
POSTOPERATIVE MANAGEMENT:
The shoulder is immobilised in a sling for three weeks (stable fixation due modern suture anchors), and passive range of motion exercises for abduction, flexion, and internal rotation are begun on the first postoperative day. After four weeks, active range of motion exercises are begun in all planes including external rotation. After twelve weeks, full loading is permitted.
See Living with a Sling and Post-operative protocol
RESULTS:
These depend on numerous factors, and optimal recovery can take over one year to achieve. Approximately 70% improvement is expected in most people after one year.
