Biceps tendon classifications
1. LHB lesions: Topographical classification
2. Biceps tendon disorders: Yamaguchi and Bindra classification
3. Biceps pulley lesions :Habermeyer, 2004
4. Histological changes in LHB tendon: Murthi
5. Subluxation of long head of biceps: Habermeyer and Walch
6. Dislocation of long head of biceps: Habermeyer and Walch
LHB lesions: Topographical classification
Hedtmann, Verlag, 2002
| Lesions of LHB | I |
SLAP lesions I-IV
Andrews lesions |
| Supratubercular lesions | II | Isolated tendinosis / tendinitis (Partial) tears of LHB (Partial) tears of LHB in rotator cuff lesions Supratubercular instability (Walch I) |
| Sulcus associated lesions | III | Subluxation / dislocation out of the bicipital groove (Walch II) without lesions of posterosuperior rotator cuff but where applicable accompanied with a lesion of the subscapularis tendon (and capsule) |
| Lesions below the bicipital groove | IV | Peripheral of proximal LHB (e.g. at tendon-muscle transition zone) |
Biceps tendon disorders: Yamaguchi and Bindra classification
In: Disorders of the Shoulder: Diagnosis and Management, Lippincott Williams and Wilkins, 1999
1. Inflammatory
a. Biceps tendinitis with cuff disease
b. Primary biceps tendinitis
2. Instability
a. Subluxation- anterior
unstable at proximal groove
following mal/nonunion of lesser tuberosity
b. Dislocation- extraarticular with partial subscapularis tear
intraarticular with full thickness subscapularis tear
3. Traumatic
a. Traumatic rupture- partial/ complete
b. SLAP lesions: Type1- significant fraying
Type 2- complete detachment of biceps and labrum
Type 3- bucket handle tear of superior labrum
Type 4- central superior labral tear with biceps extension
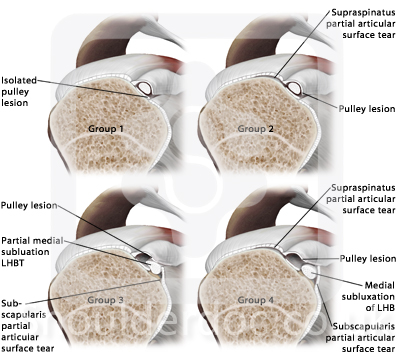
Pulley lesions (Habermeyer 2004)
Habermeyer et al, JSES, 13:5-12, 2004
Group 1: isolated lesions of the SGHL
Group 2: lesion of the SGHL and partial articular side lesion of the supraspinatus tendon
Group 3: combination of a lesion of the SGHL and deep surface tear of the subscapularis tendon
Group 4: combination of a lesion of the SGHL and a deep surface tear of the supraspinatus and subscapularis tendon
Histological changes in LHB tendon: Murthi
Murthi et al, JSES, 9:382-385, 2000
1.Normal
2.Chronic inflammation
3.Fibrosis
4.Mucinous degeneration
5.Vascular congestion
6.Dystrophic calcification
7.Acute inflammation
![]() Top
Top
Subluxation of long head of biceps: Habermeyer and Walch classification
In: Rotator cuff disorders, edited by Burkead, 142-159, Williams and Wilkins, 1996
Type 1 Superior subluxation with partial or complete tear of the rotator interval sling (the circular sling of the SGHL and coracohumeral ligaments).There may be an associated tear of supraspinatus.
Type II Subluxation at the groove. The tendon slips over the medial rim of the groove and sits upon the lesser tuberosity, with detachment of the superior portion of subscapularis.
Type III Malunion or non union of the lesser tuberosity
Dislocation of long head of biceps: Habermeyer and Walch classification
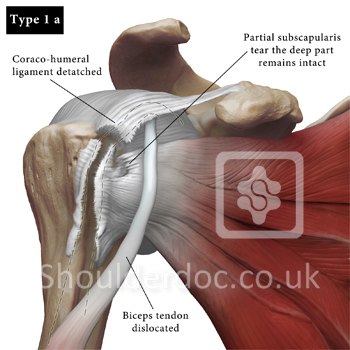
Type 1
A. Extra-articular dislocation with a partial subscapularis tear
The biceps tendon is completely dislocated and lies over the lesser tuberosity. The deep part of subscapularis remains intact. The SGHL and coraco-humeral ligaments are detached.
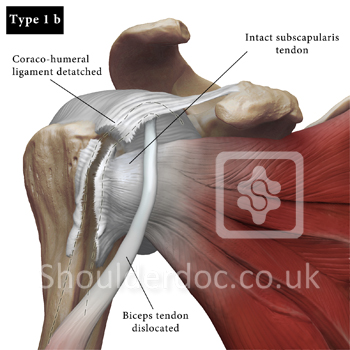
B. Extra-articular dislocation with an intact subscapularis tendon
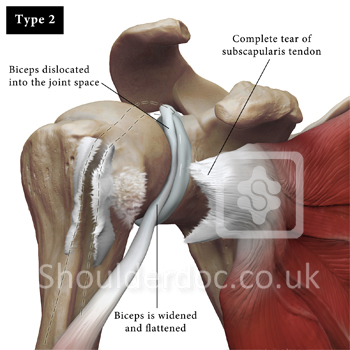
Type 2
Intra-articular dislocation of the long head of biceps combined with a complete tear of subscapularis tendon.
Biceps is widened and flattened. Subscapularis is completely torn from the lesser tuberosity ,biceps dislocates into the joint space infero-medially, associated with a cuff tear.