
HAGL Injury
HAGL = Humeral Avulsion Glenohumeral Ligament
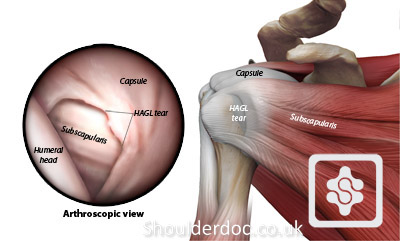
The capsule of the shoulder joint, which contains the Inferior Glenohumeral Ligament is ripped off the humerus with dislocation of the shoulder.
This is an injury that is probably associated with a higher risk of recurrent dislocations than a Bankart tear.
A HAGL tear can be difficult to diagnose and should always be suspected.
It is impossible to see on a plain MRI scan and a MR-Arthrogram or CT-Arthrogram is better. It can be seen at arthroscopy, only if the surgeon specifically looks for it as that area of the shoulder can be difficult to view with a standard arthroscopy.
Some HAGL tears can be repaired by arthroscopy, but often an open surgical repair is better to access it properly.
HAGL tear. The image on the right shows the HAGL as seen at arthroscopic surgery:

Arthroscopic Repair of a HAGL Tear:
The patient is placed onto their side or in a beach chair position, with
the operative arm in traction and slightly abducted from the side their
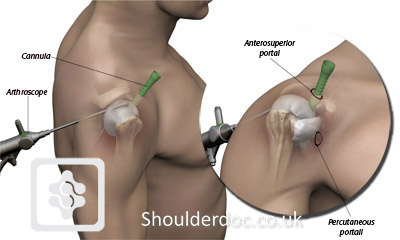
body. A posterior portal is made for the arthroscope and two anterior
portals are established for the surgical instruments. The first of these
anterior portals (superoanterior portal) is placed in the superior
aspect of the rotator interval with a clear cannula. The second portal
(percutaneous portal) a couple of centimetres directly below the first,
in a trans-subscapularis fashion, through the subscapularis tendon.
This portal is necessary for the proper angle of approach to the neck of
the humerus for suture anchor placement.
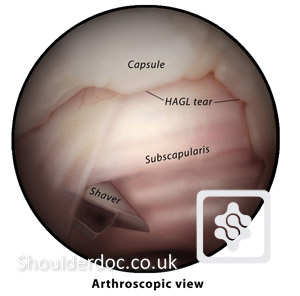
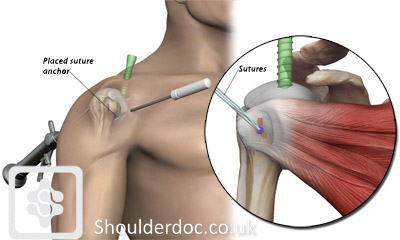
Once the portals are established, the HAGL tear is identified. In order to prepare the bony bed, the original humeral insertion site of the glenohumeral ligament complex is gently debrided using a burr shaver.
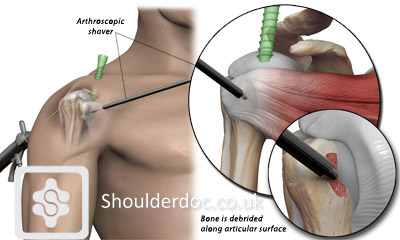
A suture anchor is placed into the medial humeral neck via a percutaneous portal through the subscapularis muscle.
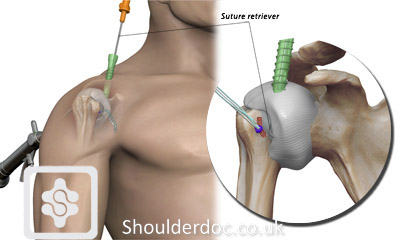
A suture retriever is advanced through the cannula and passed through the inferior/lateral capsule just inside of the avulsion borders.

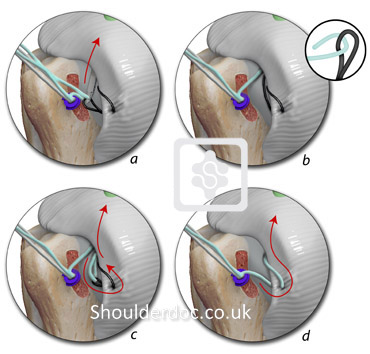
A monofilament suture loop is advanced into the joint through the suture retriever device and retrieved through the anterosuperior portal with one of the suture limbs. The remaining suture limb is left outside the skin. The monofilament is tied to the suture limb and shuttled back through the percutaneous portal through the capsuloligamentous complex, pulling the suture behind it and then out through the anterosuperior portal again.
The suture is pulled out through the percutaneous portal and a mattress suture is tied with a knot pusher. This allows for the knot to be placed outside the capsule. This can be repeated as the repair continues.
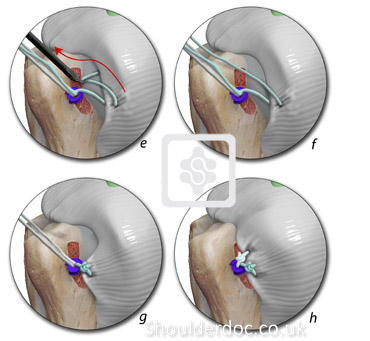
After the repair of the HAGL, examination under anesthesia is performed to verify firm anterior and anteroinferior glenohumeral stability.

The patient is placed in a shoulder immobiliser sling after surgery and rehabilitated according to the anterior stabilisation rehabilitation programme. For more details click here.
Video of arthroscopic repair of HAGL:
