
Greater Tuberosity Fractures
Lennard Funk
The greater tuberosity is the prominent area of bone at the top of the humerus and is the attachment for the two large, powerful rotator cuff muscles - supraspinatus and infraspinatus.
It is injured/fractured in a fall by either landing directly onto the side of your shoulder or landing with your arm outstretched. It may fracture alone, or with other injuries of the shoulder joint (commonly a shoulder dislocation or complex humeral fracture).
As with most fractures it may be displaced (out of its normal position) or undisplaced.

Undisplaced Greater Tuberosity Fracture (The 'hidden fracture')
I call this the 'hidden fracture' as an undisplaced fracture of the greater tuberosity is common and often does not show up on x-rays. It is common for people to injure their shoulder and x-rays look normal. This is frequently seen in skiing and mountain biking injuries. A diagnosis of 'shoulder sprain' or deltoid injury or rotator cuff injury is given and rest, rehabilitation and painkillers recommended.
If your shoulder injury is not settling in a few weeks after a fall and x-rays are normal, then you should suspect a greater tuberosity fracture. It can be very easily seen on an MRI scan and also usually on an ultrasound scan of the shoulder.

Surgery is not needed for an undisplaced fracture, but these relatively minor fractures can take a long time to heal and for the pain to settle. Shoulder stiffness and frozen shoulder is also frequent after an undisplaced greater tuberosity fracture. This may require treatment, like a true frozen shoulder. In some cases it can take up to one year to fully recover.
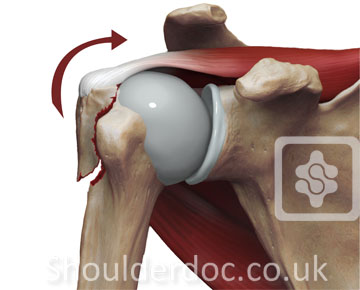
Displaced Greater Tuberosity Fracture
Isolated displaced greater tuberosity fractures are thought to occur in less than 2% of proximal humeral fractures, and are normally associated with anterior shoulder dislocations. The greater tuberosity fragment detaches with its attached rotator cuff and will characteristically have a longitudinal tear in the cuff between the supraspinatus and subscapularis tendons. The greater tuberosity fragment is pulled superiorly by the supraspinatus and posteriorly by infraspinatus and teres minor.
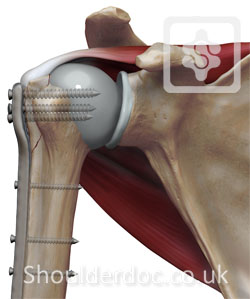
Treatment
As greater tuberosity fractures are usually retracted posteriorly and superiorly, a closed reduction is difficult. If left in position, impingement will develop against the acromion, limiting elevation and external rotation of the shoulder. However if the fracture is associated with anterior dislocation then a closed reduction of the glenohumeral dislocation may successfully reduce the greater tuberosity fracture, and once it has healed, recurrent anterior instability is unlikely.
The surgical approach to this fracture is much like a rotator cuff repair, anterosuperiorly, often complete with an acromioplasty. An alternative approach is a deltoid-splitting approach, but instead of taking the deltoid off the anterior acromion, it is peeled off the posterior acromion which avoids the acromioplasty and minimizes weakening of the anterior deltoid. This approach is especailly helpful if the fragment is displaced posteriorly. Fixation of smaller fractures can be accomplished with heavy sutures, wire or occasionally, screws. Rotator cuff tears associated with the fracture are also closed. If in the case of a large greater tuberosity fracture, a deltopectoral approach would allow for more adequate exposure for reduction and proper fixation.

References:
- MS George. Fractures of the greater tuberosity of the humerus. Journal of the American Academy of Orthopaedic, 2007
- A Green, J Izzi. Isolated fractures of the greater tuberosity of the proximal humerus Fractures. Journal of shoulder and elbow surgery, 2003
- M Zanetti, D Weishaupt, B Jost, C Gerber, J Hodler. MR imaging for traumatic tears of the rotator cuff: high prevalence of greater tuberosity fractures and subscapularis tendon tears. Fractures. AJR. American journal of …, 1999
- C Bahrs, E Lingenfelter, F Fischer, EM Walters. Mechanism of injury and morphology of the greater tuberosity fracture. Journal of shoulder and elbow surgery, 2006.
- BJ Mason, R Kier, DF Bindleglass. Occult fractures of the greater tuberosity of the humerus: radiographic and MR imaging findings. AJR. American journal of roentgenology, 1999.
- RM Patten, LA Mack, KY Wang, J Lingel. Nondisplaced fractures of the greater tuberosity of the humerus: sonographic detection. Radiology, 1992
