
Arthroscopic Lat Dorsi Tendon Transfer
Chris Peach and Len Funk
(based on the techniques of Gervasi1 and Kany2)
Latissimus Tendon transfer for massive irreparable posterior rotator cuff tears can be performed safely by a part-keyhole approach. Some surgeons feel this approach has many advantages, however the outcomes are similar to the open approaches.
Procedure details:
Preparation:
The operation is under general anaesthesia with an interscalene regional block. Patient position is supine, with the arm positioned in forward elevation in internal rotation to access the posterior axillary fold. An arm positioner (eg. Trimano, Arthrex or Spider, Smith & Nephew) is very useful for this or a secure padded mayo table across abdomen at an appropriate height.

Open tendon harvesting:
The latissimus dorsi muscle winds around the inferior border of the teres major, which also contributes to the surface marking of the posterior axillary fold. The thoracodorsal neurovascular bundle is medial to the muscle belly at this level and must be protected when mobilisation is carried out.
Identify and develop the interval between the latissimus dorsi and the teres major. Identify the musculotendinous junction at which point the tendon is very broad and thin. Dissect superiorly along the tendon edges towards the humeral insertion. Divide the tendon at the humeral attachment, protecting and avoiding the axillary and radial neurovascular structures.
Mobilisation of the muscle is performed toward the lateral border and inferior angle of the scapula. There is frequently a tether of connective tissue which needs to be released towards the scapula. Medial dissection is carried out having identified the thoracodorsal neurovascular bundle. Adequate mobilisation of the muscle is when the tendon can reach the anterior edge of the greater tuberosity.
The plane between the teres major and the deltoid is then developed to pass the tendon into the shoulder.
Arthroscopic procedure:
The arm is returned to resting position by the side, without traction.
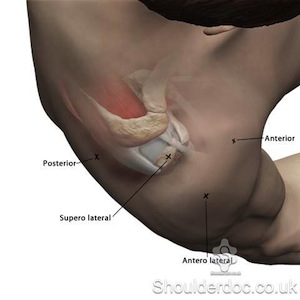
Portals used are posterior, posterolateral, lateral and anterolateral. Make a standard posterior viewing portal and clear bursal tissue to aid vision. Create an anterolateral portal, which is placed to align with line of pull of the tendon when it enters the joint from posteriorly and will be used to deliver the tendon into the joint.
Prepare footprint for tendon attachment, which is posterior to the supraspinatus insertion at the junction between that and the attachment of infraspinatus. This position has been shown to optimise function of the transfer (Favre et al. JSES 2008).
Palpate through posterior wound, in the plane already developed, onto the joint capsule. Pass a suture manipulator through the anterolateral portal posteriorly, passing superior to any remaining posterior cuff, and use it to create a rent in the posterior capsule and dilate this from outside to in. Deliver tendon into joint.
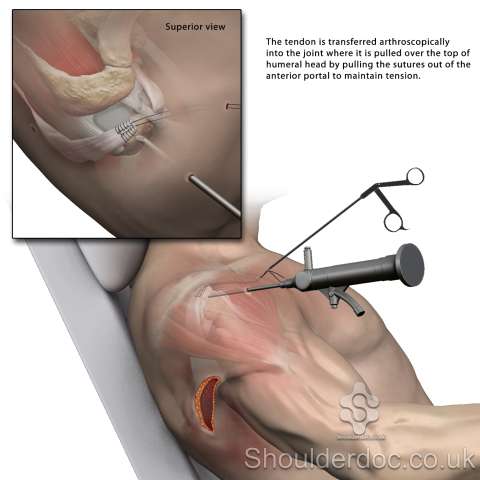
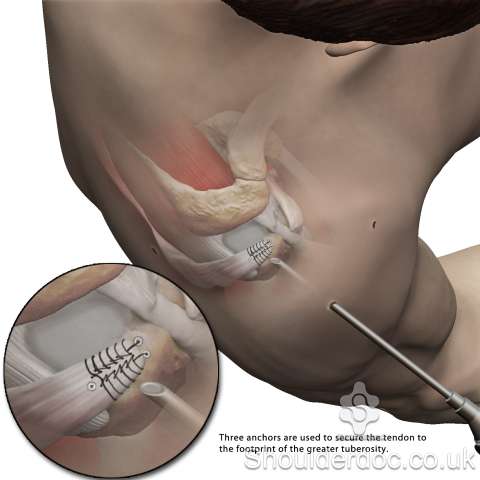
Maintain tension on the tendon with traction through the anterolateral portal on the sutures. Insert a double loaded anchor at proximal end of desired footprint and pass one limb of each suture through the tendon at this point, but leave to tie at the end. Insert a second row suture anchor loaded with both limbs from one of the whipstitch sutures at the lateral end of the new tendon footprint, and another loaded with the other sutures medial to the end of the footprint. Secure these and then tie proximal sutures.
Post-op rehab:
The shoulder is immobilised in an abduction or external rotation brace for three weeks, and passive range of motion exercises for abduction, flexion, and external rotation are begun on the first postoperative day. After four weeks, active range of motion exercises are begun in all planes including external and internal rotation. After twelve weeks, full loading is permitted. Full Rehab protocol click here.
References & Bibliography:
- Enrico Gervasi, Araldo Causero, Pier Camillo Parodi, Diego Raimondo, Giuseppe Tancredi. Arthroscopic Latissimus Dorsi Transfer Arthroscopy: The Journal of Arthroscopic & Related Surgery, Volume 23, Issue 11, November 2007, Pages 1243.e1-1243.e4
- Kany, Jean MD; Kumar, Hemanth Alladu; Chang, Vivian K.; Grimberg, Jean; Garret, Jérôme; Valenti, Philippe. Mini Invasive Axillary Approach and Arthroscopic Humeral Head Interference Screw Fixation for Latissimus Dorsi Transfer in Massive and Irreparable Posterosuperior Rotator Cuff Tears. Techniques in Shoulder & Elbow Surgery:March 2010 - Volume 11 - Issue 1 - pp 8-14
- Philippe Favre, Michael D. Loeb, Naeder Helmy, Christian Gerber. Latissimus dorsi transfer to restore external rotation with reverse shoulder arthroplasty: A biomechanical study. Journal of Shoulder and Elbow Surgery, Volume 17, Issue 4, July–August 2008, Pages 650-658
