
Proximal Biceps Disorders
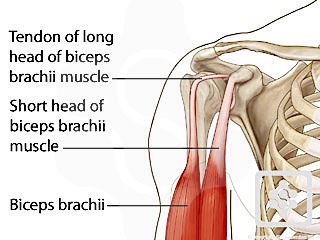
The proximal biceps comprises the short head of biceps and the long head of biceps. The short head of has a muscular and aponeurotic origin from the coracoid. Ruptures of the short head of biceps are incredibly rare and unusual. However, the long head of biceps (LHB) which arises from the superior labrum at the supraglenoid tubercle has a long tendinous portion which traverses a substantive route within the shoulder and then extra-articular before joining the musculo-tendinous junction at the level of the humeral neck. The formation of the LHB in taking this tenuous course is an evolutionary phenomenon as humans have evolved from walking on all fours to an upright stance, using their shoulders for manipulation and overhead tasks as opposed to ambulation.
As the LHB traverses from intra-articular to extra-articular it is contained within the biceps groove between the lesser and greater tuberosities by the biceps pulley (deep) and by the transverse ligament (superficial).
The biceps pulley is a key stabiliser to the biceps and is made up by the superior glenohumeral ligament and coracohumeral ligament, both being intricately associated the subscapularis tendon and the supraspinatus tendon. The biceps pulley can be easily appreciated and visualised arthroscopically, as well as during open dissection.

Biceps pulley seen at arthroscopy
FUNCTION OF THE LONG HEAD OF BICEPS
- Flexor: This role of the long head of biceps in the shoulder has been open to some controversy. It has been shown to be a minor flexor providing 7% of shoulder flexion.
- Depressor: It has a weak depression effect in association with the intact cuff depressing the humeral head.
- Stabiliser: LHB acts as a stabiliser for the glenohumeral joint only in the absence of all the other dynamic and static stabilisers to the joint. It provides an equal amount of stability as the short head of biceps. (Itoi, 1993)
- Throwing: The LHB appears to be predominantly active during the overhead throwing action. It is active only during this stage of elbow flexion and most active during deceleration of the elbow (Andrews, 1985).
LHB PATHOLOGIES
Conditions affecting the long head of biceps are:
- Tendonitis.
- Rupture.
- Biceps instability (subluxation or dislocation)
- The causes of biceps instability are due to:
- A pulley rupture
- Rotator cuff tear (subscapularis)
- Fracture mal-union on non-union
- The causes of biceps instability are due to:
DIAGNOSING LHB PATHOLOGY
Proximal biceps pain is mainly felt by the patient with any lifting activities, overhead sports activities - those activities particularly relating to lifting in the frontal plane with the elbow flexed, such as putting a box on one shoulder or also playing overhead sports such as tennis. The pain is well localised and very specific to the anterior aspect of the shoulder, in line with the long head of biceps tendon.
The clinical features are:
- Anterior shoulder pain
- Localised tenderness specifically over the biceps groove and proximal biceps
- Speeds test, which has an 80% sensitivity
- Yergasons test, which has a 50% sensitivity
- AERS test (abduction, external rotation, supination)
A LHB rupture is denoted by a typical 'popeye sign' with a dropped biceps muscle. The retracted muscle may be fixed or mobile. In my experience patients with a mobile (unfixed) ruptured biceps tend to suffer with discomfort, cramping and aching from the biceps muscle with activities.

Popeye sign
INVESTIGATIONS
- X-rays may be beneficial, particularly the axillary view showing osteophytes or malunion and bony abnormalities in the region of the biceps groove.
- Ultrasound scan is particularly helpful for demonstrating fluid around the long head of biceps dynamically assessing the stability of the biceps with internal and external rotation of the arm and also assessing the integrity of the subscapularis tendon. Abnormalities of the bone in the biceps groove can also be seen, in particular osteophytes and degenerative changes, as well as fractures and fracture mal-unions. Dislocated LHB tendon can also be clearly seen. The absence of the biceps tendon in the groove and the retracted muscle can be seen in the case of a complete LHB rupture.
Modern ultrasound scanners are also able to demonstrate intra-substance tears and tendonosis of the biceps tendon. (Armstrong, 2006). An ultrasound scan by a skilled clinician is much more beneficial for LHB pathology than MRI scans. - Arthroscopic examination is the best form of imaging for the biceps origin and superior labrum for SLAP tears the intra-articular long head of biceps is easily visualised and 1cm of the extra-articular biceps can be pulled into the joint to assess a part of the extra-articular biceps. The subscapularis, supraspinatus and biceps pulley can all be best visualised arthroscopically and also dynamically assessed.
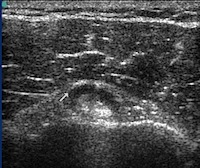
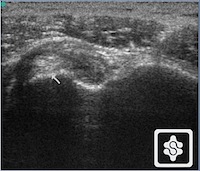
Ultrasound scans showing biceps tendonitis on the left (fluid in the biceps sheath) and a dislocated LHB on the right (arrow)
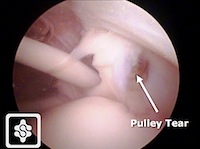
Pulley tear at arthroscopy in an overhead athlete
TREATMENT
1. Physiotherapy:
Functional biceps tendonitis can occur with glenohumeral instability, as well as scapula disorders. Instability and protraction of the shoulders leads to tension on the long head of biceps tendon. This can be addressed by postural correction and a scapula setting and stabilising regime.
2. Injections:
Injections into the biceps tendon sheath are beneficial to reduce inflammation and swelling of the biceps sheath. However it is essentially that these be performed under ultrasound guidance and my personal preference is towards Hyaluronan injections rather than corticosteroids due to the proteolytic natures of steroids and risk of rupture with corticosteroids.
3. Surgery:
- Pulley lesions are predominantly an injury of the overhead athlete and is a rare injury being a diagnosis of exclusion. Pulley lesions can in these circumstances be repaired arthroscopically.
- Biceps Tendonitis is treated either with a biceps tenotomy or Biceps tenodesis . A number of authors have published on the role of tenotomy versus tenodesis (Mariani et al, 1988; Koenig, 2004; Walch, 2005; Wolf, 2005; Osbhar, 2002; Kelly, 2005; Robert, 2005; Franceschi, 2006; Duff & Campbell, 2012). Long head of biceps tenotomy is a good treatment for biceps tendonitis but should be reserved to elderly and low demand patients only as the resulting popeye deformity and possible cramping of the muscle are a common problem in high demand and athletic patients. Biceps tenodesis is indicated for more active and higher demand patients. This can be performed as an arthroscopically assisted procedure with good strong fixation and early return to manual activities and sports.
- LHB ruptures: Most LHB ruptures cause very little symptoms and do not require treatment. However high demand manual patients and athletic patients with a mobile and stable long head of biceps rupture do often complain of cramping and aching of the biceps muscle. In these circumstances a subpectoral biceps tenodesis is of benefit (Mariani, 1988, Ng & Funk, 2012).
