
Propionibacterium acnes Infection of the Shoulder
Benjamin Kadler, Saurabh Mehta & Lennard Funk
Propionibacterium acnes
Propionibacterium acnes (P. acnes) is a non-spore-forming, anaerobic, gram-positive bacillus. It is of low virulence and therefore can be a commensal in the lipid-rich sebaceous follicles and deep layers of the skin, conjunctiva, external auditory canal, respiratory tract and intestinal tract (1, 2). P. acnes mostly colonises the pilosebaceous follicles in the skin of the upper-body, especially the head, neck, shoulders and axilla (3, 4). Pathogenic activity of the organism has, however, been shown in conditions such as meningitis, septic arthritis, osteomyelitis, chronic prostatitis and sarcoidosis. P. acnes expresses proteins required for cell-adherence, which are also antigenic and therefore capable of initiating an inflammatory response of the host’s innate immune system within the joint (1). P. acnes also secretes cytotoxic chemicals and enzymes designed to degrade body tissues, which can be harmful within the shoulder capsule (1). Furthermore, P. acnes is also able to secrete and live within an extracellular polysaccharide biofilm aiding joint colonisation and micro-colony formation, as well as avoid phagocytosis and survive macrophage engulfment (1). The combination of the bacterium’s upper-limb distribution and role in prosthetic joint infection is now forcing shoulder surgeons to consider P. acnes as an ‘orthopaedic pathogen’ (2).
Drug resistance
Patient knowledge about P. acnes is mostly limited to acne vulgaris, the skin infection present in the vast majority of young adults and teenagers (1). Hormonal changes and genetics cause sebaceous gland inflammation, dysfunction and proliferation providing an environment for the opportunistic P. acnes (1). The treatment of this skin condition with experimental courses of broad-spectrum antibiotics, often combined with poor compliance, is thought to be a contributor to antibiotic resistance (3). Gold standard antibiotics such as penicillins, vancomycin, tetracyclines and erythromycin often eradicate the bacterium, however, over half of P. acnes cultures now carry resistance to more than one of the above antibiotics (3).
Incidence and Prevalence
Over the past decade, P.acnes has become increasingly recognised as a cause of infection in orthopaedic surgery, especially when prosthesis is involved (5). With regards to shoulder replacement surgery, one study reported infection rates for primary shoulder replacement to be less than 4% but, following reverse replacement, to be as high as 18%. In this study the most common bacteria identified were Staphylococcus epidermis and P. acnes (6). However, in a retrospective review over 7 years carried out in Canada, 80 patients were identified who underwent joint cultures after primary shoulder arthoplasty and P. acnes was found to be the only significant infectious agent in 25% of participants, making it the most common pathogenic organism (7). A study of periprosthetic joint infections (PJI’s) after total shoulder arthoplasty (in the last 33 years) found that Staphylococcus was the dominant organism in the vast majority of cases, whereas, from 2001 – 2008, the incidence of P. acnes was found to be almost as high as Staphylococcus (8). This increasing incidence could be the result of changes in the microbiology of shoulder infections, heightened awareness of the organism, better surveillance or improved laboratory diagnostic techniques (8). P. acnes appears to be a prominent aggressor and is becoming more prevalent.
Risk Factors
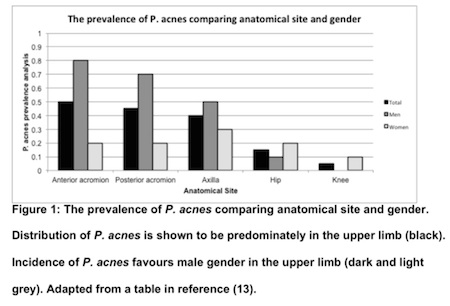
Recorded risk factors for P. acnes infection are male gender, surgery of the upper body (especially the shoulder), increased duration of surgery and, interestingly, being the first surgery of the day (3, 13). The predominance of P. acnes in shoulder infections has been linked with the presence of the axillary lymph nodes (14).
A study that involved culturing the epidermis of wounds during revision surgery, found that 16 of the 18 males involved had P. acnes infection whereas only 7 of the 12 female subjects tested positive (11). Further studies have also found that male gender and prior prosthetic implants are significant risk factors for P. acnes infection (7, 13). The male predisposition has been linked with the habitat of P. acnes being in the hair follicles and therefore the upper body of males would harbour more of the bacterium (See Figure 1) (13). Furthermore, males were found to have over 2.5 times higher risk than females after shoulder arthroplasty (15). Interestingly, if shoulder arthroplasty was performed following trauma rather than elective surgery, the risk of infection was nearly 3 times higher. Reverse arthroplasty again was shown to increase the risk of infection with P. acnes. Younger age was also identified as a risk factor, with each year of increasing age causing a risk reduction of 5%. Body Mass Index and diabetes mellitus, which are usually associated with increased risk of infection, were not found to be risk factors (15).
From the literature it is evident that patients most at risk of P. acnes infection are young people, males, those who have undergone upper limb surgeries (especially reverse shoulder replacements) and those who have surgery following trauma.
Diagnostic Difficulties
Despite laboratory and investigative advances, the diagnosis of shoulder infections due to relatively low-virulence organisms, like P. acnes, remains difficult. The non-specific clinical presentation, inadequate culture performance and the inability to accurately interpret positive cultures mean that diagnosis can be delayed (7). Research has found that inflammatory markers usually indicative of infection may not be raised in P. acnes infection (9). In 2014, in a clinic in the US, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were both raised in only 10% of patients who were identified as having P. acnes infections of the shoulder (9). In a further study, the sensitivities of CRP and ESR in the shoulder were found to be 42% and 16% respectively, whereas in the lower limbs the sensitivities for CRP and ESR were 88% and 75% respectively (10). Thus, although the sensitivity and specificity of these inflammatory markers are strong in the lower limbs, they are poor indicators of post-operative shoulder infections (9). These data fit well with the distribution of P. acnes and its indolent nature. It has been further suggested that, due to its slow growth, P. acnes needs longer culture times (up to two weeks), making it harder to spot (10). Furthermore, lowering the threshold for diagnosis (concentration of neutrophils in the tissues) would increase sensitivity because of the low inflammatory behaviour of P. acnes (10).
Clinical Presentation
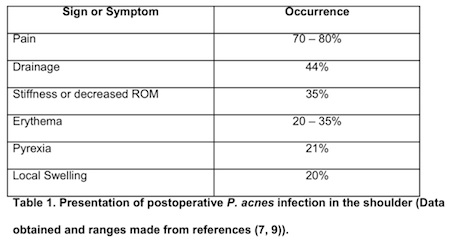
A common assumption is that the origin of P. acnes infection is in the dermis of the patient’s skin and that it travels from the surface to contaminate the surgical site (11). Surface sterilisation before surgery does not, however, eradicate the bacterium as the organism actually resides deep in the sebaceous glands. Scalpel incisions slice through these follicles, allowing for seeding and leakage of the bacteria (11). Innovative methods of sterilisation may therefore be required to penetrate the dermis and reduce P. acnes spread. Further, the need for intraoperative screening of wounds and prolonged cultures to assess the risk of developing a postoperative shoulder infection has been emphasised (11). For low-grade P. acnes shoulder infections, pain may be the only symptom, followed by stiffness with all other signs of infection being absent (12). Periprosthetic joint infections can be extremely serious and may result in loss of normal function of the joint or even progress to sepsis (6). The common patterns in clinical presentation are displayed in Table 1.
A study which focussed on postoperative pain, found that patients felt pain for an average of 3 months before diagnosis of P.acnes infection and that the mean time from surgery to diagnosis was almost 2 years (3). It was also suggested that the variance in the clinical presentation of shoulder infections may not only be due to the non-specific clinical manifestation of P. acnes, but also due to co-infection with other bacteria within the surgical site (3).
Prosthesis Failure
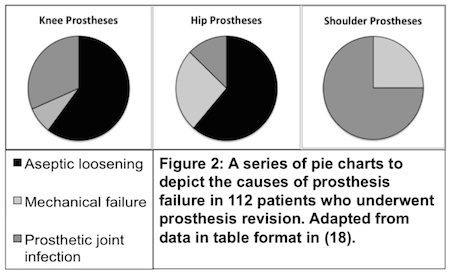
Infection is the commonest cause of joint replacement failure in the shoulder (18) (Figure 2), but aseptic loosening may be due to low grade P. acnes infection. Of the 63 cases of aseptic loosening and 63 cases of joint infection, P. acnes was found in 12 and 2 cases respectively. In cases of mechanical failure, no P. acnes was found. P. acnes should therefore be considered in cases of aseptic loosening of joint implants. The presence of P. acnes in what was thought to be aseptic loosening requires further research (18).
Treatment and Outcomes
With the increase in the number of shoulder operations and the increasing prevalence of P. acnes, advances in treatment and management of such infections has been accelerated. Superficial surface infections can be controlled using wound care and antibiotics, however, deeper infections into the surgical site may require antibiotic treatment combined with surgical removal of infected tissue (debridement). Functional outcome of the shoulder may be affected and, due to repeated surgery, there may be formation of excess scar tissue (16). Surgical debridement alone has not been shown to eliminate infection (5). A retrospective research project evaluating the characteristics and clinical outcomes of PJIs (periprosthetic joint infections) of the shoulder stated that clinical trials have provided little evidence of the best antibiotic regimes for P. acnes in the shoulder (5). Vancomycin and clindamycin are first-line for deep P. acnes infections of the shoulder; however, first-generation cephalosporins and penicillins may have a greater role in the future (5). Rifampin and daptomycin combined (to avoid rifampin resistance) have been shown to yield the highest cure rate of 63% in an animal cage model. This study also suggested that, with low-grade infections such as P. acnes, exchange of the prosthesis might provide the best clinical outcome (14).
Prevention
The increasing prevalence of P. acnes and other bacterium likely to infect during a prosthetic shoulder operation has provided a demand for innovative methods of reducing contamination. The application of a liquid cyanoacrylate-based sealant onto the skin of patients before surgery to act as a barrier for surface infection, combined with the iodine wash, has been found to reduce rates of infections compared to just the iodine wash alone (17).
P acnes and Arthritis
P. acnes may play a role in the development of arthritis of the shoulder (2). It has previously been shown that the injection of P. acnes into the joints of rats leads to arthritis and this inflammatory process may be triggered by the presence of P. acnes (2). Furthermore, there is a theory that the relapsing-remitting cycles of pain in osteoarthritis may be linked to the flare-ups of the bacterial population within the joint (2). This research was initiated due to the findings of high incidences of P. acnes in shoulders before arthroplasties, suggesting a correlation between the bacterium’s presence and arthropathy (2).
References
1. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: From acne to implant-infections, from phylotype to resistance. Medecine et maladies infectieuses. 2014;44(6):241-50.
2. Levy O, Iyer S, Atoun E, Peter N, Hous N, Cash D, et al. Propionibacterium acnes: an underestimated etiology in the pathogenesis of osteoarthritis? Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons [et al]. 2013;22(4):505-11.
3. Millett PJ, Yen YM, Price CS, Horan MP, van der Meijden OA, Elser F. Propionibacterium acnes infection as an occult cause of postoperative shoulder pain: a case series. Clinical orthopaedics and related research. 2011;469(10):2824-30.
4. Lorillou M, Martha B, Chidiac C, Ferry T, Lyon B, Joint Infection Study G. Chronic Propionibacterium acnes prosthesis joint infection manifesting as a large abscess with gas, without prosthesis loosening. BMJ case reports. 2013;2013.
5. Crane JK, Hohman DW, Nodzo SR, Duquin TR. Antimicrobial susceptibility of Propionibacterium acnes isolates from shoulder surgery. Antimicrobial agents and chemotherapy. 2013;57(7):3424-6.
6. Klatte TO, Junghans K, Al-Khateeb H, Rueger JM, Gehrke T, Kendoff D, et al. Single-stage revision for peri-prosthetic shoulder infection: outcomes and results. The bone & joint journal. 2013;95-B(3):391-5.
7. Wang B, Toye B, Desjardins M, Lapner P, Lee C. A 7-year retrospective review from 2005 to 2011 of Propionibacterium acnes shoulder infections in Ottawa, Ontario, Canada. Diagnostic microbiology and infectious disease. 2013;75(2):195-9.
8. Singh JA, Sperling JW, Schleck C, Harmsen WS, Cofield RH. Periprosthetic infections after total shoulder arthroplasty: a 33-year perspective. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons [et al]. 2012;21(11):1534-41.
9. Mook WR, Garrigues GE. Diagnosis and Management of Periprosthetic Shoulder Infections. The Journal of bone and joint surgery American volume. 2014;96(11):956-65.
10. Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. The Journal of bone and joint surgery American volume. 2014;96(6):442-7.
11. Matsen FA, 3rd, Butler-Wu S, Carofino BC, Jette JL, Bertelsen A, Bumgarner R. Origin of propionibacterium in surgical wounds and evidence-based approach for culturing propionibacterium from surgical sites. The Journal of bone and joint surgery American volume. 2013;95(23):e1811-7.
12. Schneeberger AG, Yian E, Steens W. Injection-induced low-grade infection of the shoulder joint: preliminary results. Archives of orthopaedic and trauma surgery. 2012;132(10):1387-92.
13. Patel A, Calfee RP, Plante M, Fischer SA, Green A. Propionibacterium acnes colonization of the human shoulder. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons [et al]. 2009;18(6):897-902.
14. Achermann Y, Sahin F, Schwyzer HK, Kolling C, Wust J, Vogt M. Characteristics and outcome of 16 periprosthetic shoulder joint infections. Infection. 2013;41(3):613-20.
15. Richards J, Inacio MC, Beckett M, Navarro RA, Singh A, Dillon MT, et al. Patient and Procedure-specific Risk Factors for Deep Infection After Primary Shoulder Arthroplasty. Clinical orthopaedics and related research. 2014.
16. Saltzman MD, Marecek GS, Edwards SL, Kalainov DM. Infection after shoulder surgery. The Journal of the American Academy of Orthopaedic Surgeons. 2011;19(4):208-18.
17. Lorenzetti AJ, Wongworawat MD, Jobe CM, Phipatanakul WP. Cyanoacrylate microbial sealant may reduce the prevalence of positive cultures in revision shoulder arthroplasty. Clinical orthopaedics and related research. 2013;471(10):3225-9.
18. Portillo ME, Salvado M, Alier A, Sorli L, Martinez S, Horcajada JP, et al. Prosthesis failure within 2 years of implantation is highly predictive of infection. Clinical orthopaedics and related research. 2013;471(11):3672-8.
