
Ultrasound
Ultrasound is not a technique commonly associated with orthopaedics, although interest in the technique is growing. Ultrasound of the rotator cuff was first described in 1984.[11] However, the advance of technology has been such that the development of high resolution scanners and high frequency probes, typically 7.5-10 MHz, has improved the accuracy of the technique. The advantages of the technique are that it is quick and non-invasive, and it is easy to examine both shoulders at one sitting. Images can be obtained in several different planes.
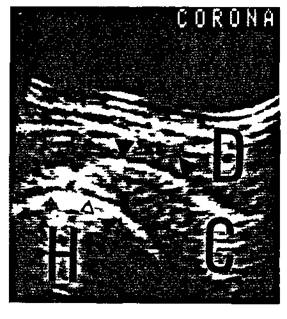
Figure 3.8 Normal rotator cuff on coronal ultrasound: right shoulder seen from in front. D = Deltoid, C = Rotator cuff, H = Humeral head.
The technique has the potential to demonstrate partial thickness tears. Figure 3.8 is an example of a normal cuff in the coronal plane, with the greater tuberosity, and the deltoid muscle lying superficially. Images are also obtained in the sagittal plane, and transversely. It is also important to observe the cuff during rotation of the shoulder. The criteria used to diagnose a cuff tear are controversial. There is general agreement that visualization of a defect, or non-visualization of the cuff as in Figure 3.9 where only the deltoid is visible, and no cuff can be seen, are reliable criteria for the diagnosis of a cuff tear.
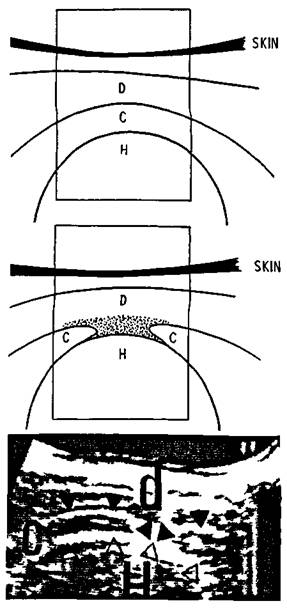
Figure 3.9 Full thickness rotator cuff tear on sonography (sagittal scan). Top shows line diagram of the normal normal appearance. Middle shows line diagram of rotator cuff tear. Bottom shows sonogram of rotator cuff tear (dark arrows top of cuff and tear, light arrows bottom of cuff). D = Deltoid, C = Cuff, H = Humeral head.
The significance of areas of altered echogenicity (Figure 3.10) is less certain. Some may represent full thickness and some partial thickness tears, but the changes are not consistent, and alterations in echogenicity alone should not be used as the sole criterion for diagnosis.[12] Areas of fibrosis or calcification can also produce abnormal echogenic areas.[13] In one prospective series of 51 shoulders, ultrasound had a sensitivity of 100 per cent for the detection of a cuff tear, but the specificity was only 75 per cent, and the overall accuracy 92 per cent. The major disadvantages of the technique are the time it takes to learn the method, and the fact that arthrography may still be required before surgery. It is sufficiently sensitive to exclude serious cuff tears with confidence in good hands.
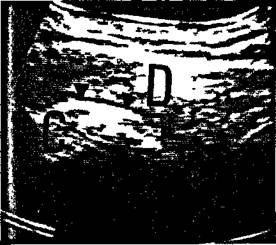
Figure 3.10 Coronal scan of left shoulder showing a highly echoic insertion of the supraspinatus tendon.
There have been reports of the use of ultrasound in the evaluation of the postoperative shoulder. This is a situation in which arthrography is less helpful, as a successfully repaired cuff may still leak contrast. Unfortunately, postoperative changes in cuff echogenicity are common, and acromioplasty removes a normal ultrasonic landmark, making it difficult to separate cuff from overlying deltoid. Nevertheless, if the criteria of non-visualization, or demonstration of a defect are used, the technique is highly accurate in the diagnosis of recurrent tears.[14]
