
Elastic Nailing of Clavicle
Elastic Intramedullary Nail treatment of displaced midshaft clavicle fractures
Nassir Naderi & Lennard Funk, 2008
UPDATE: 2018 - We do not advocate this technique for most clavicle fractures in adults. It is suitable only for simple, minimally displaced uncomminuted fractures and displaced fractures in children (rarely).
Clavicle fractures are common and the mid third of the clavicle is involved in 70-80% of cases.
Although non-operative treatment is a widely accepted treatment, delayed and poor healing occurs in approximately 10-30%. This is more common in high energy injuries, females, older patients, smokers and shortened, overlapped fractures. Fractures that heal in a shortened position can sometimes lead to unsatisfactory results such as unfavorable humping, shortening and poor shoulder function. However, this is uncommon and usually only a problem for overhead workers and athletes.

In general, operative techniques have not been widely used because complication rates are felt to be high (ranging from 5-20%). These include: wound problems (keloid scars, numb patches, superficial infections, discomfort), implant loosening, metalwork failure, non-union, infection and re-fracture after implant removal.
Plate fixation has been the standard operative fixation method, however a large strong plate is generally required to overcome the bending and torsional forces on the clavicle. Plates can therefore be prominent and superficial. There is also a stress- riser at the edges of the plate presenting a fracture risk. Plates are often removed after 18 months, especially in high risk groups such as collision athletes.
Intramedullary pinning is an attractive option which is much less invasive and avoids most of these problems. The clavicle is a long bone and shaft fractures elsewhere are usually best treated with intramedullary methods. However, historical techniques using pins or modified nails have had serious reported complications, such as intra thoracic migration and damage to the underlying structures. These were rigid devices inserted from the lateral fragment.
Elastic nails have become increasingly popular for the fixation of many long bone fractures, particularly in children. They work by providing a three-point fixation in the medulla of the bone and are not prone to the problems of previous nails and pins.
Rehm KE, et al. (Operat Orthop Traumatol 2004 Nr. 4) described a new method for intramedullary fixation of clavicle with Elastic Stable Intramedullary Nails (ESIN), using a medial insertion point and percutaneous method.
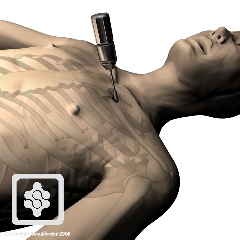
In this technique the elastic titanium nail is inserted at the sternal end of the clavicle, where the sagittal diameter of clavicle is at its maximum and there is no risk of intra thoracic migration of nail.
Surgical Technique:
The insertion point is made approximately 1 cm lateral to the sternoclavicular joint. A one centimeter skin incision is made and a hole is drilled in the anterior cortex with a 3.2 mm drill bit and guide.
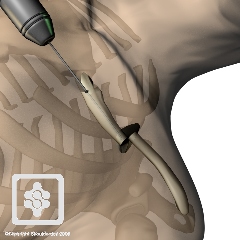
The entry portal may be enlarged with an awl and then an elastic nail (diameter between 2 to 3 mm) inserted in the medullary canal of the clavicle with a universal chuck and T-handle.

With oscillating movements the nail is advanced until it reaches the fracture site. If closed reduction is unsuccessful, an additional skin incision is needed at the level of the fracture site for open reduction of the fragments. Although the clavicle is S shaped, the tip of the ISEN is curved which helps the surgeon to pass the elastic nail into distal fragment. After adequate engagement of the distal fragment, the medial end of nail shortened and skin closed over it. The procedure is performed under fluoroscopic guidance.

It is often necessary to make a small incision over the fracture site and perform an open reduction.

Postoperatively patient is encouraged to move the arm as much as tolerated. Immobilisation is not required. We tend to limit extreme overhead activities for 3-6 weeks.
Usually callus can be seen on radiographs after 4 weeks and the nail can be removed after 3 months.


Published Results:
Rehm KE, et al [1] reported on 136 cases with average age of 32.9 years. In 60% of patients closed reduction was successful. Nails were removed after an average of 7.6 months. One hundred and six cases had a follow-up of greater than one year, all with reported satisfactory functional results. There was one nonunion, but no other significant complications. The nail was prominent medially in eight cases and required trimming. In five cases the lateral cortex was perforated, but this caused no problems. Secondary shortening of clavicle (1.5 ± 0.5 cm) occurred in 3 patients who had comminuted fractures.
Jubel A, et al [2] evaluated the efficacy of this method in 12 athletes with displaced midclavicular fractures. There were no complications and all fractures healed rapidly. The patients returned to sport 2-3 weeks after surgery. The authors concluded that the intramedullary fixation allowed rapid resumption of sporting activities.
Muller MC, et al [3] analyzed the 45 patients with a mean follow-up of 24 months. Iatrogenic perforation of the lateral cortex occurred twice and medial prominence in eight patients. Superficial skin infection developed in one. Nail breakage after fracture healing was observed twice. After 6 months the results were excellent based on the Constant and DASH scores.
Summary:
Percutaneous elastic intramedullary nailing of the clavicle is a safe, reliable method for fixation of certain displaced midshaft clavicle fractures.
It is not suitable for comminuted or old fractures and the pin does require removal at 2-3 months.
In our practice we prefer it for displaced clavicle fractures in adolescents, athletes and certain acute non-comminuted displaced fractures in adults.
References:
- Klaus E. Rehm, Jonas Andermahr, Axel Jubel; Intramedullary nailing of Midclavicular Fractures with an Elastic Titanium Nail; Eur J Traum Emerg Surg, Vol 31 Issue 4 (2005)
- A Jubel,J Andemahr, H Bergmann, A Prokop, K E Rehm; Elastic stable intramedullary nailing of midclavicular fractures in athletes; Br J Sports Med 2003; 37:480-484
- Muller MC. Burger C. Florczyk A. Striepens N. Rangger C; Elastic titanium nails in minimally invasive osteosynthesis for mid-clavicular fractures; Chirurg. 78(4):349-55, 2007 Apr
