
Normal motions of the shoulder joint
CHAPTER II
THERE are certain anatomic terms customarily applied to the motions of the joints in general which are well understood except when applied to the shoulder. For instance, will the reader kindly flex his shoulder, i.e., his scapulo-humeral joint, to its utmost. Please pose in turn in extreme abduction, extreme adduction, and in extreme extension. I plead with you to try these positions before you read any further, for it probably will be necessary for you to reeducate yourself so far as the meanings of these terms are concerned. Having determined what you think they mean, answer the following questions':
What motion occurs in the scapulo-humeral j oint when you raise your finger tips as high as you possibly can toward the ceiling?
In what position is the joint when your body is in the "anatomic" position ?
Picture to yourself a horse taking a jump. Does he flex his scapulo-humeral joint before he takes the jump or after?

FIGURE 19. HORSE TAKING A JUMP
Before reading further please name to yourself the position in which this figure shows the scapulo-humeral joint. In the man? In the horse?
There is some room for a difference of opinion on these questions, because we may be guided by the point of view of comparative anatomy or accept the terms which have become customary for the biped human. In man, the conventional anatomic position adopted for teaching purposes is a standing one with the arms at the side and the palms forward. The anatomic position for a horse is the position in which we usually see him standing, with his forelegs at a right angle with his spine. Man would have to raise his arms to a right angle in front of his body to approach the horse's position.
Sisson in "Comparative Anatomy of the Domestic Animals" (1921 edition) gives the following definitions:
"Motion which diminishes the angle included by the segments forming the joint is termed flexion, while that which tends to bring the segments into line with each other is called extension.
Circumduction. This designates movements in which the distal end of the limb describes a circle or a segment of one. In man such movement is easily performed, but in quadrupeds it is possible to a limited degree only, and is to be regarded usually as an indication of disease.
Adduction and abduction designate respectively movement of a limb toward and away from the median plane."
The horse clearly flexes his scapulo-humeral joint as he takes a jump and extends it as he lands on the other side. From a quadruped point of view we might say that the anatomic position of man is one of flexion of the shoulder; complete elevation of the arm (the Statue of Liberty or the diving position) is extension.
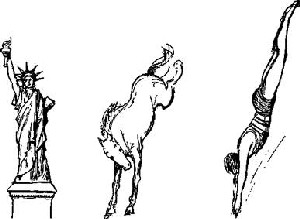
FIGURE 20. ELEVATION OF THE ARM
The term "elevation" clearly applies to the Statue of Liberty, but the arms seem to be "depressed" in the case of the diver, and it would seem absurd to use it to describe the position of these joints in the case of the horse, yet the relations in his shoulder bones are the same as in those of his human companions. A comparative anatomist would hold that all these figures represent "extension" of the scapulo-humeral joint. In this book the term "elevation" will be used for this relation of the humerus and scapula whatever the position of the body, but occasionally, to make the meaning clear, the term "extension," usually qualified by "quadruped," will be used.
From general usage in medical works, on the other hand, we think of the anatomic position as the starting point. Abduction to most surgeons probably means raising the arm to the completely elevated position pointing to the sky, and they would not specify whether this should be done in internal or external rotation, nor in what plane. Extension would probably mean to them the position assumed in enthusiastic greeting with both arms thrust forward (i.e., the anatomic position for the quadruped). When one falls in this position one is said to fall on the extended hands or arms. If you ask a surgeon to put his shoulder joint in extreme flexion he will usually flex his elbow and bring his arm forward and upward. On the principles of comparative anatomy, he should bring his elbow behind his back, or shrug his shoulder. I have several times asked audiences of doctors to rise and place their arms in flexion, extension, adduction or abduction; the results were amusing enough to convince all of us that these terms have very vague meanings, so far as the shoulder is concerned.
The fact is that the members of the medical profession have taken very little interest in this wonderful joint and do not think of its mechanism as precisely as they do of that of their favorite automobile. For the very reason that there are no standard definitions I must be somewhat arbitrary in defining the terms I shall use in this book.
When in doubt it is well to follow Gray in anatomic matters, but in this instance he avoids the issue with great skill. Gray says: " The shoulder joint is capable of movement in every direction, forward, backward, abduction, adduction, circumduction, and rotation. The humerus is drawn forward by the pectoralis major, anterior fibers of the deltoid, coracobrachialis, and by the biceps when the elbow is fixed; backward, by the latissimus dorsi, teres major, posterior fibers of the deltoid, and by the triceps when the elbow is fixed; it is abducted (elevated) by the deltoid and supraspinatus; it is adducted (depressed) by the subscapularis, pectoralis major, latissimus dorsi, and teres major; it is rotated outward by the infraspinatus and teres minor; and it is rotated inward by the subscapularis, latissimus dorsi, and teres major."
Observe that he has not used flexion or extension and thus avoids controversy. He qualifies "abducted" by a bracketed (elevated) and "adducted" by (depressed). Are the arms in diving depressed, elevated, abducted or extended?
Piersol does not help us, for according to him the diver's arms are flexed. "A motion bringing the distal end of a limb bone nearer the head is called flexion; the opposite movement, extension." If we accept this definition for the scapulo-humeral joint, flexion would occur as we raise the arm from the anatomic position to bring the elbow up beside the head, a motion which in the horse would be extension.

FIGURE 21. ABDI'CTION
The comparative anatomist would admit that the scarecrow holds its arms abducted, but he would differ with the anatomist as to the degree of abduction, and as to the plane in which the humerus had arrived at this position. The polo pony, he would contend, is in the same position as is the scarecrow; i.e., the forelimbs are carried outward from the median line as far as nature permits. The anatomist would say that the scarecrow had performed abduction for about 90° from the anatomic position through the vertical coronal plane; the comparative anatomist would insist that the motion had occurred in the horizontal transverse plane. Abduction for the comparative anatomist has reached its limit, but the ordinary surgeon would say that the arms could be still further abducted until they pointed vertically -upward at the side of the head; yet the anatomist might call this portion of the motion, flexion. Both would agree that the scarecrow's arms are abducted, and I shall call this position abduction irrespective of the degree of rotation of the humerus, or of the plane through which it is attained.
A horse or a dog may appear to abduct one leg somewhat as in the lower cut (c), but careful observation will show that most of this abduction is obtained by flexion of the elbow joint plus a little rotation of the scapula; little or no outward motion has occurred in the scapulo-humeral joint itself.
Piersol says that adduction is bringing the limb "towards the median plane of the body," yet most surgeons would, I think, consider the arm adducted when in the anatomic position at the side, as Gray says, "depressed." Suppose that Piersol had placed a student in the scarecrow position and then asked him to adduct his scapulohumeral joint. Would he mean to have the student move it upward to a position by the head; "towards the median plane of the body" or downward (depressed) to the anatomic position "towards the median plane of the body"? Certainly he could not find fault with the student who had studied his pre-medical biology and carried his arm in across his chest.


FIGURE 22. ADDUCTION
The horse, even when coaxed by a kind master, can adduct his foreleg only to a very slight extent; man himself has much less ability to adduct than he has to abduct. If the reader will try the position shown in this drawing of a traffic officer, he will be surprised to find how little true scapulo-humeral adduction occurs. Be sure not to move your scapula.

FIGURE 23. LAOCOON- ILLUSTRATES DORSAL FLEXION
The position of Laocoon's left arm is not denned anatomically in English, but it has been called "retroversion" by Braus, the German anatomist, and I have christened it "dorsal flexion."
Laocoon's right arm is not in a complete position, either from the point of view of elevation or from that of rotation.
After giving much thought to these matters, I have concluded to adopt the wise policy of Gray and avoid using the terms flexion and extension so far as I may. But what shall I call the position of Laocoon's left arm as he struggles to drag the head of the serpent from his hip? I shall want to speak of this position again and again, for it is the very position in which it is easiest to feel a ruptured supraspinatus and much the most favorable position in which to operate on such cases. Yet neither anatomists nor comparative anatomists have a definite name for it. I will christen it "dorsal flexion," although it is merely extreme flexion to a horse as he takes a jump.
What of the opposite motion? Shall we call it forward flexion or extension, or abduction, or elevation in the sagittal plane? I shall use the first when necessary but usually the last.


FIGURE 24. INTERNAL ROTATION
When the hand is placed behind the back the humerus is rotated inward to its full extent and yet lies in the same long axis which it assumes in the anatomic position; therefore, so far as the shoulder joint is concerned it may be described as in the anatomic position, but the degree of rotation should also be mentioned. The horse cannot permit his foreleg to assume this position, even with the help of the imagination of the artist, for the horse cannot rotate his humerus on its long axis.
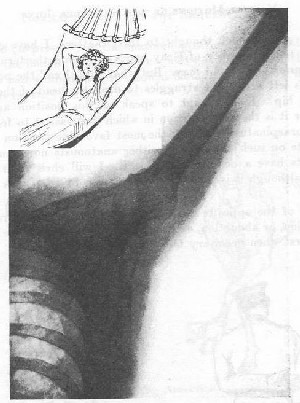
FIGURES 25 AND 26. ABDUCTION AND EXTERNAL ROTATION
This is a very natural position for the human arm when the body is recumbent. Many people sleep with one or both arms held in this manner. The scapulo-humeral joint itself has almost reached the pivotal position but the clavicle is not fully elevated. Since the deltoid, the supraspinatus and the infraspinatus are relaxed, it is the most favorable position to encourage physiological repair of lesions in and about the tuberosity.
Antero-posterior view in hammock position. Notice the symmetrical relation of the acromion to the head of the humerus. Notice that the axis of the humerus is in line with the axis of the spine of the scapula, and that changes in the relations of these axes would make different parts of the periphery of the acromion act as fulcrums. Notice that in this position the axis of the head and neck of the humerus is in the same plane as both of these axes; in other words, it points toward you at about 45° from the long axis of the shaft. If this patient raised her arm to complete elevation, with the axis of the humerus vertical, the rounded contour of the articular surface would point outward and forward, and the axis of the neck would make an obvious angle with that of the shaft.
This shoulder joint is locked, so far as posterior motion is concerned, but it still might have a number of degrees more lateral motion in the coronal plane, provided it rotated a little before it reached the true pivotal position where it would become locked. Such a position as that shown in this picture I call a subordinate pivotal position; i.e., a position in which the joint is locked posteriorly so far as dorsal motion is concerned, but lateral motion is still possible if the humerus be rotated.
Subordinate pivotal positions occur all the way from the anatomic position to that of complete elevation. They are conjunctions of the two bones in quadruped abduction with different degrees of humeral rotation. They are expressed graphically by the triangle in Fig. 29, or by the face of the clock in this diagram.
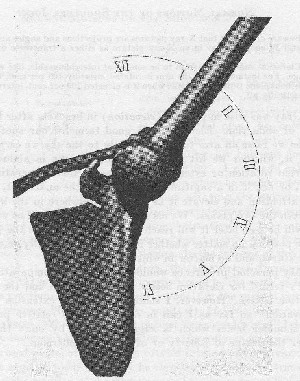
For example when the arms, are akimbo, the humerus and acromion lock, so far as motion in the coronal plane is concerned, when the axis of the humerus has reached an angle a very little over 45° from the vertical, as the patient stands. If, when in this position, the humerus be rotated outward 90° more, further elevation may be made until locking occurs at about the horizontal plane and the humerus then will be in extreme internal rotation; and although the humerus has just been rotated outward, you cannot, now that it has been raised, rotate it much inwardly! However, it will easily rotate outward 90° more, and in the coronal plane ascend to the pivotal position, where it will be almost completely locked, and the possibility of rotation in either direction will be very slight. On the way to this complete locking it will pass this neutral position, which I have called the hammock position, and in which the joint and its adjacent structures are very nearly at rest. In this position the X-ray shows the facets of the teres minor and of the subscapularis in profile, and the axis of the humerus points at one-thirty on the dial of the acromion.
All of this goes to show that the scapulo-humeral motions cannot be determined by experiments on the cadaver with the scapula held in a vise, for the humerus moves in different ways according to the position of the scapula. Furthermore, not only the subtle changes due to rotation of the humerus on its long axis, and the still more subtle changes in the shape of the coraco-acromio-glenoidal cup while the clavicle rises, but changes in the position of the spine, must be considered to attain a true understanding for clinical purposes. Tell me how many degrees of elevation of the humerus the scapulo-humeral joint permits; then put your hand behind your back and demonstrate it to me! You are in a subordinate pivotal position at about six o'clock on the dial of the acromion. Contrast this with the motion when you raise your arm in external rotation in the coronal plane. If you are young and limber, the axis of your humerus, when in superior posterior adduction, may precede noon on the dial of the acromion, and when in inferior posterior adduction it may pass six o'clock.
Beware of the fact that X-ray pictures are projections and angles are deceptive. A metal W could appear in an X-ray picture as either a transverse or a vertical line.
Elevation and rotation seem to be somewhat interchangeable, like wattage and voltage. For instance, when the arm is rotated inwardly 100 per cent, elevation in the coronal plane is practically nil; when it is elevated 100 per cent, internal rotation is practically nil.
Gray was wise in putting (elevation) in brackets after his definition of abduction. Elevation is a good term for our special needs. When we raise an arm to point directly to the sky we certainly elevate it, whether we lift it in the coronal plane in abduction and external rotation or extend it according to the comparative anatomist, or flex it in a sagittal plane to please the anatomist, or divide our attention and elevate it as we may, anywhere in the 90 degrees between the two planes. We may even keep it adducted as we raise it. As will be seen later it will reach in complete elevation the same ultimate position no matter whether it is rotated internally or externally as it starts, and no matter in which plane it rises.
My personal preference would be to use the comparative anatomist's terms, for elevation seems to me extension and the anatomic position flexion. However, I shall avoid using "extension" and use "elevation" so far as I can in describing the relative position of the shoulder bones which is suggested alike by one's thought of either the Statue of Liberty or of Annette Kellerman.

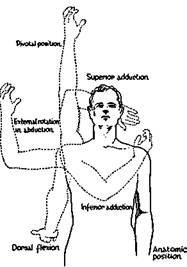
FIGURE 28. THE TERMS TO BE USED IN THIS BOOK
Should this man bring the right arm in its lower phase, which is "dorsal flexion," directly forward in the sagittal plane, he could not arrive in the pivotal position without rotating his humerus inward for about 90°. I prefer to call the motion in which he would endeavor, without rotating the humerus, to raise his arm forward in the sagittal plane "elevation in the sagittal plane," but it may be called forward flexion. In the extreme of this position, the axis drawn through the condyles of the lower end of the humerus would be the same as in the anatomic position, i.e., transverse or coronal; in the pivotal position this axis changes 90° {i.e., becomes sagittal), and the inner condyle points forward. When I say that a patient "elevates his arm" I do not especially indicate whether he rotates it externally and carries it up in the coronal plane, or whether he rotates it internally and carries it up in the sagittal plane. Usually he elevates it in some intermediate plane, and the rotation of the clavicle and of the humerus on their long axes occurs without his knowledge or observation. The only justification for using "forward flexion" is that it is the opposite of dorsal flexion, which is true extreme flexion as in the jumping horse. Forward flexion is really only extension.
Adduction would be used to describe a mid-position between " superior adduction" and "inferior adduction" of the scapulo-humeral joint. These terms may be further qualified by stating whether they are posterior or anterior. They are characteristic motions in youth, and it is remarkable to what a degree they may persist in some adult women. One rarely finds a laboring man who can perform superior adduction; many cannot even attain a vertical position.
We have by no means settled the terminology which should be used in describing the motions of the shoulder, but we have, I hope, arrived at a fair understanding of the terms to be used in this book.
Now that we have the terms to use for descriptive purposes, we may study the motions of the shoulder under the following headings:
(1) Rotation on the long axis of the humerus.
(2) The relative parts played by the three different joints in the motion of elevation.
(3) Lateral elevation in the coronal plane.
(4) Antero-posterior motion in the sagittal plane.
(5) Circumduction.
(6) The motion at the acromio-clavicular joint.
(7) The scapulo-humeral rhythm in which all the structures cooperate.
Rotation on the long axis of the humerus. When the patient is standing in the anatomic position, with his arm at the side and the palm forward, the humerus is in almost a mid-position between internal and external rotation. By turning the palm as far as one can outward, the humerus has moved to extreme external rotation. By turning the palm inward until it has faced backward and again outward, the plane of the palm has traversed nearly a complete circle (360 degrees), owing to rotation of the humerus and scapula (180 degrees), plus rotation of the radius (nearly 180 degrees). When one reaches up as high as possible, the humerus arrives at a fixed position where it can no longer be rotated, although the palm will turn nearly 180 degrees. Now in all of these motions, the turning of the palm is deceptive, because the palm turns almost a half circle by the motion of the radius over the ulna—the rotation of the humerus on its long axis being only a part of the motion. In order to get rid of this deception in testing the scapulo-humeral motion, one should flex the forearm to a right angle, and retain it in this position throughout our tests. Since the elbow joint does not move laterally, one can discount the motion of the palm and judge the rotation of the humerus (and scapula) by the angle through which the flexed forearm (i.e., the ulna) moves inward and outward. No matter what position the palm assumes, the motion of the humerus is not affected so long as the forearm is flexed at a right angle, but when the elbow is extended the humerus may rotate synchronously with the radius without our perception.
Keeping the forearm flexed at a right angle and keeping the elbow at the side, one can rotate the humerus from the anatomic position outward about 90 degrees. Keeping the elbow at the side and placing the flexed forearm behind the back, one can rotate the humerus inward about 90 degrees. The total arc of rotation, therefore, is at least 180 degrees in a normal person of medium age, provided that the arm is at the side in the anatomic position, for the degree of rotation diminishes as the arm is elevated (p. 44). This estimate is not perfectly exact because the whole scapula rotates a little also. It is slightly in excess of 180 degrees in young people, particularly in girls, and is slightly beneath this in elderly persons —although occasionally, elderly persons, particularly women, retain a large range of motion.
I wish to warn the reader not to get the idea that rotation of the humerus is a motion which occurs in the true shoulder joint only. The subacromial bursa, particularly its subcoracoid portion, is as essential in rotation as in upward motions of the arm. (See Fig. 33.)
And now we come to a curious paradox which I have only recently observed, although I have studied the motions of the shoulder for years. You can prove that the completely elevated arm is in either extreme external rotation or in extreme internal rotation.
(1) Proof that it is in external rotation.
a. Raise your hand as high as you possibly can toward the ceiling.
b. Without moving the humerus, flex your elbow to a right angle, and your forearm will lie across the top of your head.
c. Holding your elbow still flexed at a right angle, let your
humerus descend slowly, without rotation on its long axis in the
coronal plane to the side of your body.
d. The forearm will be pointing directly outward from your
body in extreme external rotation of the humerus.
e. Since you let it descend, without rotating it at all, it must
have been in external rotation all the time. Q. E. D.
(2) Proof that it is in internal rotation.
a. Raise your arm to complete elevation.
b. Flex your elbow to a right angle and the forearm is again
over your head.
c. Let the humerus (without rotating on its axis) descend
in the sagittal plane.
d. The forearm will be across the front of your body point
ing to the opposite side; i.e., in internal rotation of the humerus.
e. Since you let it descend without rotating it at all, it must
have been in internal rotation all the time. Q. E. D.
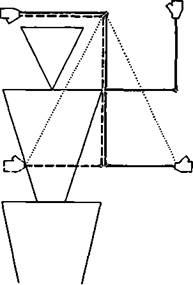
FIGURE 29. THE PIVOTAL PARADOX.
A diagram to illustrate the pivotal position and the diminution of the possibility of rotation of the humerus as the arm ascends from the anatomic position. If external rotation is performed in the anatomic position the arm may be raised in the coronal plane, as illustrated by the solid line. If it be rotated internally while in the anatomic position it can be raised in the sagittal plane, as illustrated by the dash line. The triangle completed by the dotted lines indicates the degrees of the ability of the humerus to rotate, as the arm proceeds upward. Notice that in whatever plane the arm is elevated the flexed forearm arrives .at a position over the head, where scapulo-humera] rotation practically ceases.
Still another point has been formulated only recently. The range of rotation of the humerus diminishes as it is elevated.
In the anatomic position at the side the extent of rotation is roughly 180 degrees; when raised to the level of the shoulder in abduction (i.e., the scarecrow position) or in mid-forward flexion (i.e., the normal quadruped anatomic position), it is about 90 degrees, and in complete elevation it is practically nil, for the humerus cannot be further rotated externally or internally. The loss of range is gradual between these points.
I find it difficult to explain the paradox of the ability of the elevated arm to descend without rotating and come at will to the side in either external rotation or internal rotation. It makes the puzzle more clear to hold a humerus in your hand and observe that the lines of bearing made in these two motions on the articular surface would meet each other. Also you may see that the glenoid surface comes to a point at its upper extremity. However, this does not answer the question of whether the completely elevated arm is to be considered to be in external or internal rotation. I favor internal rotation because the internal condyle points forward, but will call it a pivotal position to make sure. From the pivot it can descend in either way.
Analysis of relative parts played by the three joints during elevation of the arm. Elevation of the arm may occur in many different planes and the behavior of the scapula and humerus varies somewhat in each plane.
The rotation of the humerus on its axis, which we have just been considering, occurs in either plane if we start from the anatomic position. As has just been pointed out, in complete elevation the humerus arrives in a pivotal position in which little, if any, rotation is possible. When one reaches upward in any plane, three joints move. (1) The scapula rises on the chest wall owing to about 45 degrees of motion at the sterno-clavicular joint. (2) The acromion tilts upward under the tip of the clavicle owing to about 5 degrees of motion at the acromio-clavicular joint. (3) The humerus moves on the glenoid about 140 degrees.
Notice that the sum of these somewhat doubtful and variable figures is greater by 10 degrees than the one fixed and readily observed amount of 180 degrees, which the vertical axis of the humerus has passed through to become inverted. In other words, the full extent of motion in each joint has not been used.
In childhood and in youth the axis of the humerus may pass the vertical and proceed toward the median line at either end of its course for about 20 degrees.
Possibly by some feat of mathematics these motions may be accurately measured in the future, but the sum of the ranges of vertical motion possible in each joint will always be greater than the total of range accomplished when they all move together.
The explanation of this paradox lies chiefly in the facts that (1) each of the bones rotates in its relation to the others; (2) the clavicle also passes backward; (3) there is lateral movement as well as elevation of the two movable centers of motion; i.e., the outer end of the clavicle may pass backward while the glenoid moves forward. (4) Each joint is capable of a greater degree of motion than it uses in the combined motions required to elevate the arm.
If you will hunch your shoulder and then elevate your arm you may feel the outer end of the clavicle drop, pass backward and rotate slightly in a left turn. In other words, the clavicle can be raised higher by hunching than by elevating the arm. Rotation of the clavicle, slight as it is, tends to throw the glenoid forward and face it more directly upward. Consider that the clavicle is a rod fastened near its end to the coracoid and acromion which join together firmly at the glenoid. Forget the rest of the scapula. Twist the clavicle, which is about 7% inches long, a few degrees on its long axis, and the glenoid, which is offset two inches, will move a good deal even assuming no acromio-clavicular motion.
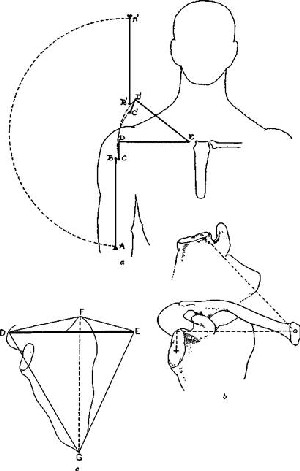
FIGURE 80. ELEVATION OF SCAPULA
NORMAL MOTIONS OF THE SHOULDER JOINT 47
FIGURE 30
Strictly speaking, any motion of the arm should be described in two ways; e.g., stating the degree of abduction of the clavicle and also the degree of abduction of the humerus on the scapula. Usually when there is abduction of the scapulo-humeral joint there is, at the same time, abduction at the sterno-clavicular joint, but this is by no means always true. We may, for example, adduct the clavicle, and at the Same time abduct the humerus. However, for clinical purposes it is best to consider the arm and shoulder as a whole. The diagrams on p. 46 suggest some of the phases of the cooperative movements of all the shoulder bones.
A—lower end of humerus. B—upper end of humerus. C—glenoid. D — outer end of clavicle. E—inner end of clavicle.
To elevate the arm straight toward the ceiling so that the axis of the humerus becomes inverted; i.e., travels 180°, three joints are used. The clavicle E-D does not move directly up to E-D', for, as it rises, it passes backward and at the same time twists anticlockwise on its own long axis about 45°. There is a negligible amount of motion at D in the acromioclavicular joint, but the rotation of the clavicle carries the offset glenoid forward and upward; i.e., the motion of D' is backward away from the plane of the paper, but the motion of C is at the same time coming forward toward the plane of the paper. Meanwhile the humerus A-B is constantly moving on the movable center C. When we subtract the upward motion of the clavicle, i.e., 45°, from the obvious 180°, we have about 185° of scapulo-humeral motion.
But how about the offset glenoid, which has also moved about 45° by rotation of the clavicle? If B and C were firmly united, A would be raised halfway to the level of C merely by this rotation. This would subtract 45° more from the 135°, leaving only 90° of pure scapulo-humeral motion. Thus authorities may disagree on the true amount of scapulo-humeral mobility according to whether or not the glenoid is considered to be fixed or in motion. It seems to the writer that the movement is cooperative and cannot be fairly subdivided among the three joints.
(6) In complete elevation, the scapula rises in nearly "one piece" with the clavicle. It is not quite "one piece," because its union with the clavicle through the coraco- and acromio-clavicular ligaments permits a certain amount of motion, the extent of which is so slight that we may ignore it in the interpretation of this diagram, which is particularly planned to suggest the idea that the motions of the clavicle are transmitted to the scapula, not only in elevation, but in rotation. However, the slight mobility of the joints between the scapula and the clavicle permits exaggeration of any one position when force, active or passive, is applied to the limb in that position.
The axes of the clavicle, the glenoid, the blade of the scapula and the acromion meet one another at varying angles, although in the main at about 45°. It is well nigh impossible to construct a diagram which would be actually correct in its attempt to show the complicated normal movements which may take place among these irregularly shaped bones meeting at such angles.
(c) If the reader will experiment with a block of wood shaped like a three-sided pyramid, the apex of which, D, represents the tip of the acromion, and the base, E-F-G, the lines drawn from the upper and lower angles of the blade of the scapula to the center of the sterno-clavicular joint, he may obtain a very good idea of the effect of any movement of the edge which represents the axis of the clavicle, whether that edge be raised or rotated. Such an experiment will make him thoughtful in regard to the X-ray interpretation of lesions of the shoulder.
The plane of the glenoid meets nearly all the faces of the pyramid at about 45° to 60°, and in the anatomic position it also assumes about this relation to the sagittal and coronal planes of the body. Place your pencil point at the center of the glenoid in this figure and hold the axis of the pencil at 45° to the plane of the paper and perpendicular to the plane of the glenoid. Then imagine rotation and elevation of D-E, and conceive of the effect on the axis of your pencil still held in the same relation with the glenoid.
The heavy line D-E is the border which represents the clavicle. Rotation of D-E for 45° on the point E shortens the X-ray projection of F-G and of all the other lines. It raises the plane of the glenoid 45° and therefore the axis of a humerus, which we may assume is moving on the glenoid. Meanwhile elevation of the clavicle for 45° raises the projection of the humerus 45° more.
When we discuss the pure scapulo-humeral motion shall we consider the plane of the glenoid to be fixed or in motion? Even without using the clavicle, tilting that plane by the use of your spine or by bending a knee makes a great difference in the relation of the long axis of the humerus to the floor.
As the arm is elevated it is very easy to feel on your own shoulder that the scapula not only rises but rotates on the chest wall. The lower angle which is easily palpated may travel an arc of over 45 degrees on the circumference of the chest. Part of this motion is made possible at the acromio-clavicular joint, but most of it is due to rotation of the clavicle at the sterno-clavicular joint.
To sum up, we may say that during the motion of elevation the humerus is rotating on its own vertical axis, pivoting on a fulcrum which is rotating and passing forward in relation to a center which is rising, moving backward and slowly rotating on a left turn.
Taking all these facts into consideration, it is quite possible that by astronomic calculation from motion-picture X-ray films of a living skeleton, the "relativity" of these compound motions might be made out. But when this has been done, calculations for the motions of the spinal column must be added, for in life it is scarcely possible to move the shoulder without compensatory curving or twisting of our spines. This is particularly true in patients with sore shoulders.
Lateral elevation of the humerus in the coronal plane cannot be accomplished as far as a right angle with the axis of the body, if the arm is first put in internal rotation {i.e., arms akimbo). However, if it starts in the anatomic position it may be raised to the horizontal or perhaps a little higher without any external rotation. This includes motion of the scapula on the chest wall through motion at the acromio-clavicular joint and at the sterno-clavicular joint. Only a part of this 90 degrees is performed by the shoulder joint, perhaps less than a half. Full lateral motion or elevation in the coronal plane can only be accomplished in external rotation. In internal rotation, the tuberosity meets the acromion, but as the arm is externally rotated, the shape of the head and neck under the acromion changes, and the head rolls in under the acromion by a very narrow margin at just about the region of the bicipital groove. At the same time the scapula tilts so that the glenoid turns upward. However, elevation in the sagittal plane can be accomplished in internal rotation.
So far as antero-posterior motion of the humerus in a sagittal plane is concerned, i.e., when the patient brings the elbow as far backward (dorsal flexion) and then as far up and forward as possible (forward flexion or elevation in the sagittal plane), the range is also nearly 180 degrees, being greater forward than backward. This is an important motion to remember, for one can palpate much more of the head of the humerus forward of the acromion when the elbow is carried as far backward (Laocoon's left arm) as possible. In this position the range of palpability of the head of the humerus is greater in some subjects than in others, depending on the shape of the acromion process and the position in which they habitually carry their shoulders. Sloping shoulders are more difficult to palpate in dorsal flexion than are square shoulders.
When the arm is carried as far forward and upward as possible in the sagittal plane, the entire humeral head, tuberosity and all, disappears beneath the acromion; the arm will be elevated to about 45 degrees above the horizontal and cannot be rotated further outward. Then if it is rotated about 45 degrees inward it will rise the remaining 45 degrees to complete elevation. But if the arm is elevated in the coronal plane it will have to be rotated outward to attain complete elevation. The bronze Mercury of Bologna shows the right arm in forward flexion, while Laocoon's right arm is abducted in mid-rotation. The former would have to rotate inward to attain complete elevation, while the latter must rotate outward.
In other words, complete elevation of the arm from the anatomic position in a sagittal plane is not possible; in order to arrive at complete elevation the humerus must rotate on its long axis externally at the start of this motion or internally at the latter part. As a matter of fact, in raising one's arm, one is unconscious of this rotation of the humerus on its long axis. Although the humerus can only rise to within 45 degrees of complete elevation in the anterior phase of this motion in the sagittal plane, it can proceed 45 degrees farther backward in the posterior phase than it can when it is rotated externally. Therefore the long axis of the humerus in the whole anteroposterior motion can also pass through an arc of 180 degrees, but the semi-circle described by the lower end of the humerus ends at a lower level in front, and passes further behind the body, than if elevation occurs in either external or internal rotation. As in motion in the other planes this movement, too, is partly accomplished by rotation of the scapula on the chest wall; that is, by motion at the sterno-clavicular joint.
Circumduction is a deceptive motion in the shoulder. One can swing the arm around and persuade oneself that the humerus is moving like a spoke in a wheel. Watch a man circumducting his arm and you will swear that the arm is rotating round and round with its hub at the shoulder joint. You do not observe that he is rotating his body, that his clavicle is circumducting through a small circle, that the scapulo-humeral joint is a moving pivot at the point of a cone, and that the humerus is rotating on its own long axis as it passes around the periphery of a compound cone, centering at the sternoclavicular joint.
It will be a good mental exercise for the reader to trace on imaginary coronal, sagittal, transverse, median and equatorial planes the points he can touch with the tip of his elbow. Or he may employ a mechanical draughtsman to plot the points on the inside of a sphere which his elbow may reach without bending his spine. He will be surprised to find how like a conventional shield this figure will be.
We may roughly say that the tip of the elbow can be made to touch any point within most of a small hemisphere, and that the elbow cannot touch any part of what would be the opposing hemisphere. If the elbow and wrist are allowed to move, a still larger portion of a sphere can be swept by the hand. Then if you will allow your spine to rotate and bend, you can very nearly sweep the inside of three-quarters of a globe.
The acromio-clavicular joint. The exact manner of, and the exact amount of motion in this joint, still elude my curiosity. When one hunches the shoulder, the scapula rises several inches on the posterior ribs, and the spine of the scapula rises to a higher level than does the clavicle; i.e., the scapula rolls forward. At the same time the angle between the spine of the scapula and the clavicle (as seen from above) appears to diminish to some extent. Furthermore, the vertebral border of the scapula remains only about 15 degrees off its normal parallel with the axis of the vertebral column, and yet the angle of the vertebral border with the clavicle as seen by X-ray diminishes. These facts all indicate that in hunching the shoulder there must be 5 or 10 degrees of motion at the acromioclavicular joint. Incidentally you will find that the clavicle rises considerably higher when you hunch your shoulder than when you reach upward.
However, X-rays of a completely elevated arm show very little change in the right angle which the vertebral border forms with the clavicle, as compared to the angle in the anatomic position, although in elevation the vertebral border has reached an angle of 45 degrees with the spinal column. If the reader will make a little model of sticks, using one for the clavicle, one for the vertebral border and one for the spine of the scapula, he may understand that a very slight rotation at the sterno-clavicular joint may greatly change the relations of the other bones as seen in any X-ray proj ection, without any movement taking place at the acromio-clavicular end. After reading various works on anatomy and making some observations by dissection and checking with the X-ray, I have come to the conclusion that the acromio-clavicular joint moves very little indeed, but this motion may occur in many different planes. Its surfaces slide a little, rotate a little, tip apart a little and act like hinges to some degree.
It appears that nature abhorred a perfectly fixed fusion at this point in her architectural plan, for it would oblige a very small point to bear the stress for a whole extremity. So she compromised by fixing the scapula near the outer end of the clavicle, by binding the latter firmly to the coracoid process and using the acromio-clavicular joint to steady the protruding tip of the clavicle on the acromion process. She bound the tip of the clavicle which extended an inch or two beyond the coracoid to the side of the acromion, not to its very tip. The ligamentous binding of coracoid to clavicle, though very strong, would- not be truly rigid; the acromio-clavicular joint must take up the play or be rigid, and if rigid, be very much subject to injury. Therefore nature made it slightly movable in order that it might: (1) Swing a little (as seen from above downward—p. 10, Fig. 6) so that the angle between the axes of the scapula and clavicle could be slightly diminished or increased. (2) Rock a little (as seen from the side) so that the lower angle of the scapula could follow the curve of the ribs as it moves about them when the scapula proceeds forward and backward. (3) Twist a little so that the face of the glenoid can point a little more upward when the arm is elevated. (This occurs with No. 2.) (4) Slide a little inward when pressure is made on the outside of the shoulder. (5) Act like a hinge when the shoulder is shrugged.
All these motions are very slight in degree and checked by the ligaments which bind the coracoid to the under side of the clavicle, more than by the relatively weak capsular ligament which surrounds the acromio-clavicular joint itself. In other words, the range of the acromio-clavicular joint is only the range of the pliability of the coraco-clavicular ligaments themselves, which are very cunningly arranged to bear the stresses which occur in any of the directions in which the joint can move.
Owing to the obliquity of the joint itself, force coming from below the acromion ( for instance, if the lower angle of the scapula were pulled forcibly outward or upward as by passively raising the arm in internal rotation in the coronal plane) would throw all the stress on the coracoid ligaments. In the same way, force from behind the acromion makes supporting contact in the joint because the clavicular surface faces backward as well as downward. These considerations are important in a study of the mechanism of dislocation.
The greatest weakness of this little joint seems to be to downward force applied to the acromion without touching the end of the clavicle which, however, protects it by projection above it. Fortunately, none of the ordinary uses of the joint subject it to a strong downward force, but a blow or a fall on the tip of the acromion without at the same time striking the clavicle, commonly ruptures the acromioclavicular ligaments without tearing the firmer conoid and trapezoid strands.
On the whole, although the acromio-clavicular joint may move a little in any direction, and is necessary for perfect shoulder motion, it has a very slight range in any direction, and may be ankylosed without- serious alteration of the use of the shoulder. It contains an intermediate fibro-cartilage which is often incomplete and sometimes absent.
The scapulo-humeral rhythm. There has been a great deal written in anatomic text books and journals, and also in articles concerning fractures a'nd dislocations in this region, about the successive stages in the motion of abduction or elevation. I have never yet found what seemed to me an accurate description.* Authors divide the motions into primary and secondary. They say, for instance, that the humerus first moves on the scapula and then the scapula on the chest wall, and later the humerus on the scapula again. My own opinion is that in the normal motion of elevation no one can tell just when each of these motions occurs, for they all occur simultaneously. This is the way to prove this statement.
•Footnote. Since writing this chapter, I have found an admirable article by an English anatomist (R. L. Lockhart), from which the following paragraph is quoted:
"In raising the arm from the side to the vertically upright position, from the very beginning to the very end of the action, there is continuous movement of the scapulo-thoracic, acromio-clavicular and sterno-clavicular joints, and continuous activity of the associated muscles, whereas traditional teaching, by authors of repute, past and present, holds that abduction of the arm to the horizontal is secured by the full action of the deltoid causing complete movement of the shoulder joint, subsequent vertical elevation of the arm being made by trapezius and serratus rotating the scapula up on the chest, while the humero-scapular angle remains constant." (Movements of the Normal Shoulder Joint. R. L. Lockhart, M.D., Jour. Anat. (English), 1929-30, Vol. 64, p. 298.)
Watch the back of a thin, naked man and concentrate your attention on the motion of the vertebral border of the scapula from start to finish of elevation, performed slowly. You will find with your finger on the vertebral border that you must follow the scapula continuously during the whole period of motion and that this motion does not occur in a jerky, but on the contrary, in a perfectly steady manner. Incidentally, therefore, the scapula cannot be performing its function in an independent way in relation to the shoulder joint. Next, concentrate your attention on the shoulder joint, with your fingers so placed that they can feel the motion of the head of the humerus on the scapula, and you will find that the motion of this joint, too, is symmetrical and steady throughout the whole of elevation. Still further, you will find that the motion is steady, whether accomplished from the start in internal rotation, or external rotation.
Now concentrate your attention on the sterno-clavicular joint. It, too, moves steadily through its special arc. The clavicle not only rises, but it passes backward and rotates, so that although its motion is oblique, it is steady throughout the whole period of elevation.
Then concentrate your attention on the level of the top of the shoulder relative to the other one that does not move. It, too, rises smoothly and continuously.
Therefore, Q. E. D., if each movement is steady and continuous, each joint is moving pari passu, although the arc of one, the scapulohumeral joint, is much greater than that of the others and attracts your attention fully three times as much. After seeing many shoulder cases, one must conclude that this rhythm of motion as the arm is elevated is the normal action. When you see a scapula that halts and does not move symmetrically the probability is that that shoulder is abnormal. Almost all lesions of the shoulder joint and bursa exhibit this sign which I speak of as "loss of scapulo-humeral rhythm" in many places in the text. (See p. 147.)
At this point it seems wise to pause for a review. Most of the motions to which I have called attention are perhaps novel to the reader. You must try these motions for yourself and verify them or disprove them. Be fair to me. It is not only necessary to try them, but to try them accurately, and accuracy is very difficult, for in spite of good intentions you may make unconscious auxiliary motions. For instance, it is almost impossible to hold one's spine rigid as one moves the arm into extreme positions. One must also be very careful to maintain the specified positions very precisely. In studying rotation, for example, one may allow the forearm to relax from its position at a right angle with the humerus, and without this guide, a very slight degree of rotation may occur which would permit greater freedom in elevation. Furthermore, it is next to impossible to disassociate movements of the scapula itself from the scapulo-humeral motions. In spite of one's will, the scapula will move a little on the chest wall and will give a deceptive freedom to the humerus. You think, for instance, that you can, with the humerus in internal rotation, perform abduction of the scapulo-humeral joint as far as the horizontal, but as a matter of fact, the degree of scapulohumeral abduction will be very meager. If your scapula were nailed to your chest in the anatomic position, I doubt if your arm could move 45 degrees from your side.
To recapitulate, I believe it is important to understand that: (1) the humerus is in external rotation when the arm is at the side and the palm turned as far as possible forward and outward; (2) a considerable scapulo-humeral adduction (quadruped flexion) is possible on the part of the patient, so that the angle of the spine of the scapula and the axis of the humerus reduces some 20 degrees; (3) reaching as high as possible (elevation) does not mean the extreme degree of "extension" of the shoulder, for some degrees more may be gained by lowering the arm back of the head toward the other shoulder; (4) the young patient has so much greater motion in all directions than does the man or woman above middle age; (5) the sterno-clavicular joint functions more in shrugging than in elevation; (6) in elevation the clavicle moves upward and backward and rotates at the sterno-clavicular joint; (7) there is only a slight degree of motion at the acromio-clavicular joint, which is not very important (many times this joint becomes ankylosed in laboring men, without special pain or disability, and motion is not seriously interfered with) ; (8) a spiral motion is made by the humerus as it ascends, rotating and rising at the same time; (9) the motion of the hand at the wrist does not involve the use of the shoulder joint, and yet when the arm is straight out by the side, the humerus usually rotates without our perception; (10) in the normal subject the scapula, the humerus, and the sterno-clavicular joint move in a rhythm so beautifully coordinated, that they all perform a steady elevation of the arm at the same time; (11) with the forearm flexed to a right angle on the humerus and raised in the coronal plane in extreme internal rotation, the humerus cannot rise quite to a right angle with the body, and that as soon as the forearm is thrown into external rotation, the humerus is in a position in which it can be elevated 90 degrees more; (12) trying to watch the three bones at once, one necessarily shifts his gaze, but in the meantime each point is still moving, and the scapulo-humeral motion, being three times as great in its arc as either of the others, attracts most of our attention, for the speed is also three times as great.
I think it is not generally appreciated that the shoulder joint is unique in so many ways. Compare its simplicity of construction with its most complicated muscular mechanism. It may be likened to the universal joint in an automobile so far as its function is concerned, but its anatomy is more simple; i.e., it is a rounded knob, loosely fitting on a small, shallow, slippery fulcrum. It is dependent for its accuracy of motion in every direction on a group of muscles which must be absolutely coordinated and always work together to some extent, each in turn acting as stabilizers, and each becoming at times the dominant muscle which either the intellect or blind habit may order. Moreover, each muscle must be prepared to substitute for a neighbor in case of slight injuries or all together to go on strike until the injured one is healed. Each and all must be able to play their parts with the greatest speed under all conditions, and at all angles as the moving fulcrums change positions.
Have you ever tried to back an automobile with a trailer attached? The usual connection with a trailer is about as simple a mechanism as is the human shoulder joint. When you back your trailer your brains take the place of the neuro-muscular apparatus of the shoulder. You back perfectly straight and the trailer goes back straight for a moment, but instantly may swing to the right or left. You correct this by swinging the rear of your car in the opposite direction and find your trailer at once going too far in the other way. Now the mechanisms of the muscles of the shoulder are more alert than we are; they could back a trailer behind another trailer. Here is an illustration of the mechanical problem when you reach up and put your finger on the ceiling. Pressing your finger up is like backing an auto with eight trailers.
Through all these motions the subacromial bursa is in constant use. It is in fact a joint without articular cartilages but quite as indispensable. When its surfaces are thoroughly adherent, half the extent of elevation is lost and nearly 140 degrees in rotation and the same amount in dorsal and frontal flexion. Rupture of the supraspinatus tendon destroys the even convexity of its hemispheric base and wrecks the normal scapulo-humeral rhythm. Soreness at the insertion of this tendon or in the bursa produces spasmodic locking of the joint.
From what has already been said in this chapter, it is apparent that the shoulder motions can be divided pretty sharply into the motions of the scapula on the chest wall and the motions of the arm on the scapula. In the former set of motions, the subacromial bursa and the supraspinatus tendon are not brought into play, for they could be made with an ankylosed shoulder joint, but in the motions of the scapulo-humeral joint, constant use is made of the bursa.
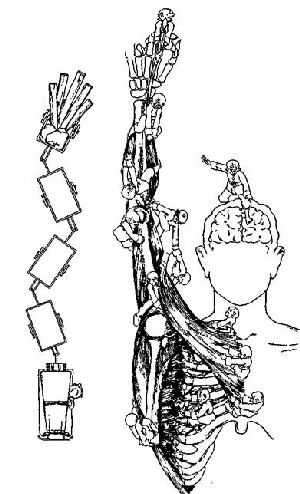
PLATE I. COOPERATION OF ALL MUSCLES
PLATE I
A man can undoubtedly raise his arm until he has reached a point as high as seems to him possible, and then with an effort he can push directly upward against that point. We may compare the mechanics of this process with the automobile and trailers shown in this diagram. Even if a driver succeeded in backing these trailers as accurately as suggested, we cannot conceive of his getting them in a line sufficiently straightened to enable him to push backward on some other object. Yet man can, without effort or strain, perform this miracle by the alignment of the bones of his arm in such a manner that a further contraction of his muscles will straighten the line of his bones and transmit the force directly away from its base.
The right-hand figure suggests a comparison with the work of a rigger who is erecting a complicated arrangement of spars, which at the final moment he can raise to a vertical position by the unanimous cooperative efforts of the crew in charge of each portion of the structure. When we consider that in each muscle, the gnomes at work are thousands, each operating a special muscle fiber, it fills the mind with admiration of the accomplishments of evolution, but with humility with regard to man's ability to undertake to know in detail such a delicate mechanism. Have we even a right to attempt gross adjustments?
A surgeon who deals with shoulder cases cannot understand these points too well, because in the most serious forms of injuries about the shoulder, he must always have the choice between recommending fixation of the joint and an excision of the joint. Excision permits rotation below the level of the shoulder so that the patient can put his hand in the opposite pocket, in front and behind his body. In fact, a patient with excision of the shoulder can turn a door-knob behind his back better with the injured arm than he can with the well one. As compensation for this mobility in rotation, he lacks the power to raise weights in abduction which is possessed by the man whose shoulder is ankylosed, who can lift with great strength within the arc of motion which he still retains; i.e., to a little higher than the level of his shoulder.
Unfortunately the clinical fact is that between these two extremes there is no halfway station. Patients with shoulder joints which are partly damaged are usually worse off than either patients with flexible excised joints or those with stiff ankylosed joints. Patients who have had excision or ankylosis soon come to a painless condition with the definite limitations spoken of above. On the contrary, if the scapulo-humeral joint is imperfect and works irregularly, it is apt to be more useless and troublesome than either the ankylosed or excised joint, because it is not only mechanically imperfect but painful, and pain creates spasm which destroys the normal scapulohumeral rhythm and inhibits effort. Thus a joint with a few degrees of motion is usually worse than one without any. When a shoulder is injured in a way to destroy its wonderful mechanical perfection, it is apt to go from bad to worse, and while in the beginning it may have a fair degree of motion short of normal, it sooner or later tends toward ankylosis.
Prognosis in shoulder conditions is therefore very important. If one is able to recognize at once those cases which will eventually become ankylosed, and separate them from those which are sure to get well, it will be of great advantage to patients who might suffer through many months and years only to end with a stiff joint. When the soft structures of tendons or ligaments only (as in bursitis or rupture of the tendons) are injured, permanent ankylosis will not occur and repair may be hoped for; but if the articular surface of the humerus itself is injured or destroyed by disease so that it becomes even partially adherent to the soft parts, practical ankylosis is almost sure to follow. It is for this reason that operative treatment of complicated fractures of the shoulder joint is so unsatisfactory, and has been a discouraging field for surgical endeavors. Such operations to be successful must be done immediately after the accident. Every surgeon should know well the respective advantages and disadvantages to be expected from excision or from ankylosis of this joint. In general, patients who must do heavy work with the arm are better off with ankylosis, while excision is preferable in those of the white collar class.
Fortunately ankylosis does not occur from rupture of the supra-spinatus tendon, for the excess of fluid which develops in these cases prevents adhesions, and although the cartilage may be exposed to friction and be eroded, it does not become adherent.
We have hitherto been considering the motions of the skeletal part of the shoulder without attempting to determine the parts played by the individual muscles in more detail than given in the quotation from Gray on page 4. There is, however, a certain obligation for me to attempt to describe the special part played by the supraspinatus. For this purpose I present two diagrams with the accompanying text from one of my former papers.
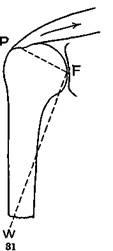
Figure 31—Showing how power is applied by supraspinatus.
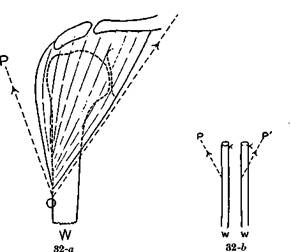
Figure 32—Showing how power is applied by deltoid
"In explaining this subject to students I find that many do not realize that during abduction (elevation) of the arm the greater tuberosity actually passes beneath the acromion and coraco-acromial ligament. They appear to think that the motion is limited by the impingement of the tuberosity on the acromion. I think this false conception is due to the usual method of articulating skeletons used for anatomic study, which does not allow the tuberosity to pass under the acromion. The diagrams (Figs. 31 and 32) illustrate the importance of the supraspinatus as an abductor. It is generally supposed that the deltoid is an abductor of the arm, but I believe it can be shown that the deltoid is not an abductor unless accompanied in its action by the supraspinatus. The deltoid alone tends to press the head of the humerus up under the acromion process.
A consideration of Figures 31 and 32 will demonstrate the importance of the function of the supraspinatus in abduction of the arm. In Figure 31 is shown how the supraspinatus applies its power on the short arm of the lever P. F. A mechanically perfect sliding fulcrum is obtained on the glenoid.
In Figure 32 is analyzed the application of the power of the deltoid to the point 0. If the power were applied by the outer fibers O-P, a fulcrum could not be obtained on the glenoid but would be obtained on the acromion, which, since it is not provided with articular cartilage, is obviously unfitted for this function. On the other hand, if the power were applied by the inner fibers 0-P', the glenoid could only act as a fulcrum in adduction. The resultant of the action of all the fibers tends to drive the head of the bone directly upward under the acromion.
When, however, both muscles act simultaneously, the power applied by the supraspinatus furnishes a fulcrum for the power of the deltoid. (Fig. 17-a.) As the lines of force of the two muscles approach one another (Fig. 17-b) the deltoid is able to obtain a fulcrum on the glenoid. In normal action the glenoid bears all the weight, and the power oi the supraspinatus keeps the tuberosity from seeking a fulcrum on the acromion and coraco-acromial ligament. The function of the bursa is to avoid friction at this point.
Soreness in the bursa, or of the tendinous insertion of the supraspinatus, throws the latter out of action and the deltoid alone cannot perform abduction. Duchenne has reported a case of circumflex paralysis where the supraspinatus alone was strong enough to perform abduction. A similar case is reported on p. 393.
The combined action of the two muscles is so habitual that one cannot voluntarily disassociate them in abduction, although one frequently uses the power of the deltoid alone to raise or square the shoulder, and vice versa, in lowering the shoulder to the position of round or sloping shoulder, one abducts the scapula on the humerus by using the supraspinatus. Even in the latter motion one cannot disassociate contraction of the deltoid."
As the years have passed I have seen no reason to withdraw any of the above statements, and I have seen many individual cases which confirm and illustrate the importance of these observations. I have seen a number of cases which confirm the observation of Duchenne, that the supraspinatus alone can perform abduction. This is referred to in Chapter XII, p. 393. On the other hand, every case of rupture of the supraspinatus confirms the remarks in regard to the function of the supraspinatus in furnishing a fulcrum for the deltoid. All cases of rupture of the supraspinatus illustrate the tendency of the deltoid to lift the arm on its vertical axis.
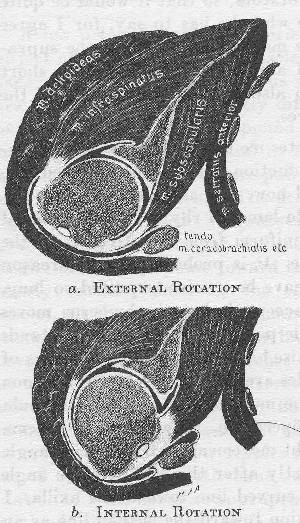
FIGURE 83. ROTATION IN THE SHOULDER JOINT
A semi-diagrammatic drawing by Mr. Aitkin from a frozen section taken transversely through a right shoulder joint. One is surprised to see how bulky the muscular mass of the shoulder seems from this point of view. One may also understand, from observation of the attachment of the serratus, how easy it is for the scapula to rock forward or backward; in other words, to rotate on its vertical axis. This rotation occurs so readily that it is difficult to determine the actual share which the scap-ulo-humeral motion performs when the humerus is rotated on its vertical axis in the anatomic position. In these diagrams the scapulo-humeral motion is indicated as about 90° between external rotation (a) and internal rotation (6), but these are probably not the extreme positions which the joint is capable of assuming. The range is probably nearly 180° in young subjects.
The diagrams illustrate the mobility of the peripheral parts of the bursae and joint. The bursa subscapularis becomes part of the joint in external rotation and the bursa infraspinati unfolds in internal rotation. In a similar way the sub-coracoid portion of the subacromial bursa rolls out in external rotation, while in internal rotation its loose periphery forms a nictitating fold as indicated here by a sharp angulation just external to the cora-coid and which corresponds to the front view shown in Figure 49. These nictitating folds occur in other portions of the periphery as well, and are quite variable in position. When the bursa is blown up or injected they largely disappear.
While it is very interesting to speculate on the exact action of any one muscle or group of muscles related to the shoulder, one must constantly bear in mind that the actions of these muscles vary greatly according to the tension in the surrounding muscles. To study the action of the supraspinatus alone, without considering the combined actions of all the short rotators, would be short-sighted. Nor can we consider the action of all the short rotators together without taking into account the positions of the whole shoulder blade on the chest as maintained by the muscles which stabilize it on the body. J. H. Stevens (Amer. Jour. Med. Sc, Dec, 1909. "The Action of the Short Rotators on the Normal Abduction of the Arm.") has discussed in a very interesting way the relation of the action of the supraspinatus to the other short rotators, so that it would be quite unnecessary for me to repeat here what he has to say, for I agree with him almost to the letter. He maintains that while the supraspinatus has the functions which I allude to above, the other short rotators have an important action also in holding the head of the humerus from below. In this I agree.
Stevens in the above article quotes me as holding that the supraspinatus initiates the motion of abduction. If I have expressed myself thus, I have changed my mind now, and as stated on page 52, I at present believe that the scapulo-humeral rhythm in elevation of the arm and shoulder together is uniform from first to last, all the muscles cooperating to some degree. It is probable that the reason that the motions of the shoulder have been misinterpreted so long, i.e., that it is almost universally accepted that the humerus moves before the scapula, is a simple little point. When the model stands erect preliminary to the order to raise his arm so that the motions of the bones can be observed, his muscles are relatively relaxed. As soon as his mind obeys the order, all the muscles related to the scapula have to work in some degree in cooperation. The very first observable motion in the scapula is a slight movement of the inferior angle toward the vertebral column. Shortly after this, the inferior angle proceeds slowly and steadily in a curved line toward the axilla. I interpret the little preliminary motion toward the median line as an effort of the secondary shoulder muscles to fix the scapula so that the short rotators and muscles of the arm can begin to work. The phenomenon may be just as well interpreted in the reverse way; that is, that the sudden assumption of scapulo-humeral action throws weight on the scapula and therefore tips the inferior angle toward the back bone. It does not seem important to decide which of these sets of muscles first begins to operate, but it is important to know that there is this little hesitation at the beginning of the motion, for I think that it is this brief period of preliminary stabilization of the whole shoulder which has led to the deception that the humerus begins to move on the scapula before the scapula begins to move on the body. At any rate, I feel quite certain that the supraspinatus must exert its power before the deltoid can act as an abductor, and that in a normal person abduction of the scapulo-humeral joint is due to a combined effort of the two muscles. As reiterated in other places in this book, I am also sure that elevation can be freely and haltingly performed, even when the supraspinatus has been evulsed, for the other short rotators can to a certain extent hold the head of the humerus on its fulcrum, the glenoid.
A few principles should be briefly emphasized before leaving the subject of the action of the muscles about the shoulder. In the first place many of the muscles in this region are fan-shaped, and therefore their fibers pull in greatly different directions. The trapezius, for instance, is really a compound muscle. Each bundle of fibers is almost a separate muscle and in fact the extreme ones are almost antagonistic. The lowest fibers pull the shoulder down and the uppermost pull the shoulder up. The deltoid itself is fan-shaped, with the edge of the fan curved. The subscapularis, infraspinatus, latissimus dorsi and pectoralis major and minor are also fan-shaped. All the handles of the fans point toward the head of the humerus. How extremely sensitive must be the cooperation between these varied muscles, all the parts of which must act together in almost any motion which we perform with our hands, for not only are the various nerves which we know as branches of the brachial plexus concerned, but the subdivisions of these nerves after they have proceeded to the individual bundles of muscular fibers. In raising the arm, for instance, a ripple of impulses must run through the bundles composing the trapezius, and similar ripples must take place through the fan-shaped origins of the latissimus dorsi, serratus, pectorals, etc. Relaxation of some fibers at appropriate moments is quite as important as stimulation of others. In fact, as one makes the simplest motion to raise the arm to touch a point on the wall with the finger, there must be a perfect symphony of cooperating relaxing nerve impulses harmonizing witli contractions from various other groups of muscle fibers, which, if analyzed in detail, would be more complex than the music written for a whole burst of harmony from an orchestra.
In studying the motions of the shoulder one must always bear in mind the serratus, the action of which is concealed. It is of great importance and is necessary to complete elevation of the arm. Remember that the majority of the animal world walk, run and leap on their serrati, for they have no clavicles to make skeletal contact.
I do not intend to attempt to review in detail the action of the other individual muscles about the shoulder. At best I could not equal the wonderful descriptions of their actions written by Duchenne in his "Physiologie des Movements," published in Paris in 1867 and remaining unsurpassed today. He was greatly interested in the study of the paralyses of these various muscles, and his analysis is much influenced by this point of view. More recently Mollier has published his lectures addressed to art students (S. Mollier, Plastische Anato-mie, Verlag von J. F. Bergmann, Miinchen, 1924). I have been able to find no contribution of importance in the literature during the 60 years that intervened.
Curiously enough, neither of these writers shows any interest in the subacromial bursa, which I regard as an indispensable part of the human joint. They do not mention it. I have frankly given all the space I can spare on anatomy to my own point of view to bring out what I feel is the relative importance of the bursa, compared to the joint itself. I have tried to show that the destruction of either joint or bursa takes away not only the motions which quadrupeds possess, but most of those remarkable additional features of the mechanics of the joint which have come to us and to the monkeys to fulfill the need for abduction and adduction.
I have described in these two chapters some aspects of shoulder motion which I have not seen mentioned elsewhere, but Duchenne and Mollier have between them covered about everything else now known about this joint, including a great deal that I have not alluded to above.
We simply must close this chapter, for there is no end to the beautiful complexities of motion which this joint performs, but if the reader has not understood and agreed (or rationally disagreed) with what I have said here, he had better not finish the book.
REFERENCES
Acknowledgment has been made in the text to the works of Duchenne, Lock-hart, Mollier, and Stevens.
