
Anterolateral Approach for Trauma
Lennard Funk & Mark Webb
Click Here for original article
The patient is placed in a beach chair position.
The bony landmarks of the corocoid anteriorly, the AC joint/anterior tip of the acromion laterally and the spine of the scapula posteriorly are identified
The operators hand is placed over the shoulder , with the middle finger over the spine of the scapula and the thumb on the corocoid, the index finger on the AC joint.
A longitudinal incision is then made in line with the index finger, starting over the anterior acromion running distally down the deltoid for 5-7cm from the lateral edge of the acromion. 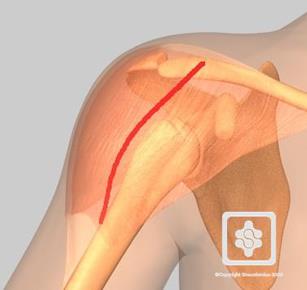
The raphe between the anterior and middle deltoid is identified and split in the line of the fibres distally for approximately 5cm (approx 1 hand`s breadth) from the edge of the acromion, to avoid injury to the axillary nerve.
A stay suture can be applied to the distal deltoid split to avoid potential damage to the axillary nerve. Beneath the deltoid the remnants of the subacromial bursa are seen and excised.
For improved proximal exposure around the head fragments, perform a subperiosteal detachment of approximately 1-2cm of the anterior deltoid insertion on the acromion. An anterior acomioplasty is then performed. 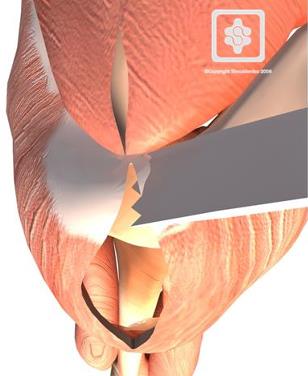
These dissections then gain direct access to the rotator cuff and insertions onto the tuberosities and proximal humeral shaft.
The fracture fragments can now be identified and mobilised back to their correct positions. If displaced, the greater tuberosity fragment will be found lying posterio-superiorly under the acromion in line with the pull of the supra/infra supinatus, teres minor, the lesser tuberosity with subscapularis is typically antero-medial. 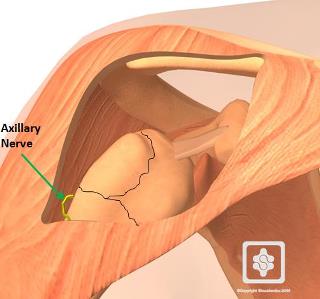
To mobilise the tuberosity fragments and gain improved exposure of the head fragment - identify the rotator interval and split the interval in line with the cuff fibres.
In 3 and 4 part proximal humeral fractures, the head fragment is typically noted to be lying medially and facing superiorly..With the fracture fragments identified , the tuberosity fragments can be secured using by passing a suture through the tendinous insertion of the cuff onto tuberosity. If the head is to be preserved, it is then elevated and reduced to it`s correct position.
By reducing the tuberosity fragments behind the head and suturing them together , the head fragment is usually secured in it`s correct position.
Once all fragments are reduced and secured, a plate can then be applied to the lateral side of the humeral head/shaft.
If more distal exposure down the humeral shaft is required, the axillary nerve is actively identified within the deltoid, mobilised and protected, allowing a plate to be slipped underneath the nerve.
Fracture fixation with a plate and screws or hemiarthroplasty can then proceed as normal.
On completion of internal fixation or hemiarthroplasty, if the the anterior deltoid has been detached, repair of the muscle back onto the acromion is required, we usually use a PDS on a short J needle . Otherwise no deep closure is required. Tacking sutures are applied to the deltoid and the skin is sutured.
Our Results
Our Results
Using this approach, we have performed 25 (23 for acute fracture, 2 for non-union) internal fixations of the proximal humerus and 19 stemmed arthroplasties for humeral head fractures. Pre-operatively all 44 patients had documented normal motor function of all three parts of deltoid muscle with intact sensory function of axillary nerve. At an average of 3 months postoperatively, patients underwent specific axillary nerve and deltoid function assessment using both clinical examination and neurophysiological study of the axillary nerve involving seperate needle EMG assesment of the anterior, middle and posterior deltoid bundles. Results from this combination of clinical and neurophysiological examination confirm that there have been no cases of axillary nerve dysfunction as a direct result of the approach or subsequent fracture fixation. There have been no cases of superficial or deep infection and no scars have been revised.
