
Move
Active movements
Active movements are assessed first. The patient is asked to elevate the shoulder to demonstrate any limitation of movement or painful arc. If movement is limited then an examining hand placed on the scapula during active elevation will show whether the limitation is glenohumeral or scapulothoracic, or both. A painful arc may be more marked with elevation in abduction rather than flexion. With the elbow locked into the side active external rotation is compared with the unaffected arm, and finally active internal rotation is assessed by comparing how far up the spine the thumb of the affected arm will go compared to the normal side. For this latter test, elbow function must be equal on both sides.
Passive movements
Elevation, external rotation and internal rotation are again measured with the surgeon holding the distal humerus in one hand and the inferior angte of the scapula under the palm of the other hand. The range, pattern of movement, end point, excess over active movement and degree of pain are all noted.
Rotator cuff strength
The clinical test of rotator cuff function is an integral part of every examination of the shoulder.
The supraspinatus test
This test (Figure 2.10) is carried out with the patient standing. With the elbow straight, the arm is placed in 20 degrees of abduction and flexion, and the patient is told to hold it there. The examiner assesses the strength of abduction, and the patient reports the amount of pain produced by this manoeuvre. The examiner then tests the opposite normal shoulder for comparison. Weakness on testing denotes a rotator cuff tear. Unfortunately, if there is a lot of pain, then weakness will be apparent due to pain inhibition, and the test will have to be performed after an impingement injection test.
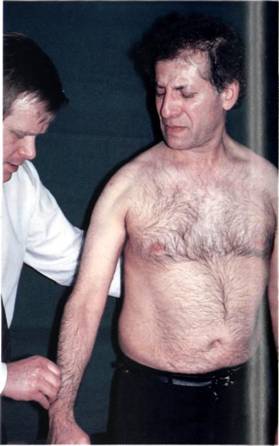
Figure 2.10 The supraspinatus test: active resisted abduction at 30 degrees tests supraspinatus strength.
The impingement injection test
This test allows the surgeon to establish whether subacromial impingement is causing the painful arc. For the test, 5 ml 1 per cent lignocaine (US: lidocaine) is injected under the anterior edge of the acromion. After 10 minutes the patient is re-examined, and if the painful arc is improved or abolished, then the site of pain has been established.
The infraspinatus test
This test (Figure 2.11) is very similar to the supraspinatus test, and is a test of resisted active external rotation of the shoulder. The infraspinatus is the only efficient external rotator of the glenohumeral joint. Pain and weakness are sought, weakness denoting a rotator cuff tear.
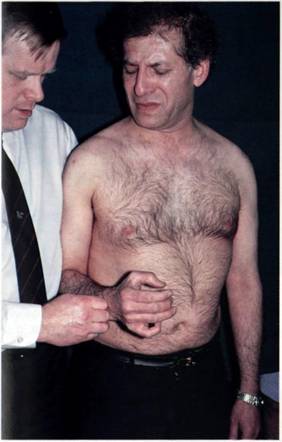
Figure 2.11 The infraspinatus test: active resisted external rotation with the elbow flexed to 90 degrees and the humerus at the side. Pain and weakness may denote a tear of infraspinatus.
The subscapularis test
This test (Figure 2.12) is similar, but opposite, to the infraspinatus test. With the elbow locked against the patient's side active resisted internal rotation of the glenohumeral joint is tested. Unfortunately this movement is produced by pectoralis major and latissimus dorsi, as well as subscapularis, and therefore is not such a sensitive test.
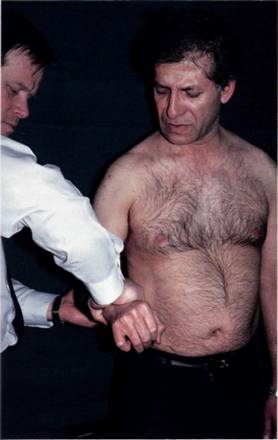
Figure 2.12 The subscapulars test: active resisted internal rotation of the glenohumeral joint.
