Surgical Approaches
The surgical approach is included in the description of individual operations within the text of this book. However, the major surgical exposures are described here, and the majority of shoulder operations may be carried out through these exposures.
Anterior Approach (Extended Deltopectoral)
The anterior approach, or extended deltopectoral approach, is suitable for total shoulder replacement and open reduction and internal fixation of proximal humeral fractures.
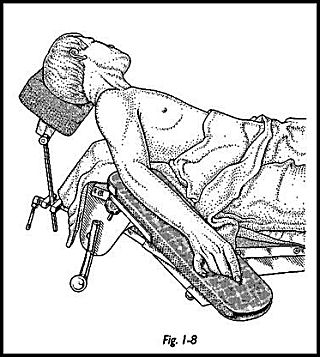
Position of Patient Positioning of patients for shoulder surgery is extremely important as the shoulder joint is the most mobile joint in the body, and by careful positioning of the limb, the joint's exposure may be kept to a minimum. The patient is placed supine with an arm board at the side. A neurosurgical head piece is preferred because this leaves access to the shoulder both posteriorly and anteriorly should any unforeseen circumstances arise that necessitate a combined anterior and posterior approach. A sandbag is placed under the medial border of the scapula to protract the shoulder forward and give better exposure of the glenoid (Fig. 1-8).
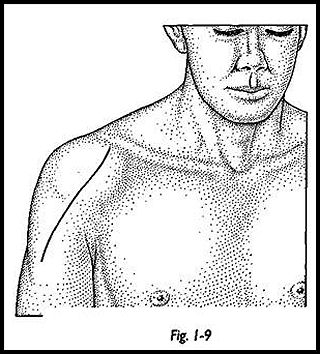
Technique The incision extends from the outer end of the clavicle lateral to the cora-coid following the medial edge of the deltoid muscle. The deep fascia is incised in the line of the skin incision, and the cut edges are swept back with a swab to identify the deltopectoral groove. The groove is marked by the large cephalic vein, which forms a useful landmark (Fig. 1-9).
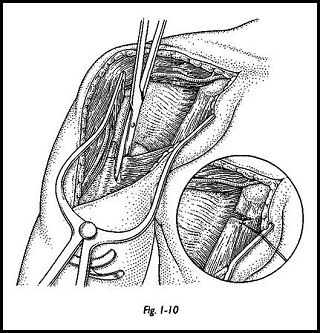
The two muscles are separated by a finger or blunt dissection, and the vein is retracted medially with the pectoralis major. A few small tributaries entering the vein from the outer side may need to be divided. Preservation of the cephalic vein is preferred if possible, as this may reduce postoperative swelling. Sometimes, however, it may need to be divided for access. A self-retaining retractor is used to separate the pectoralis major and the deltoid, and the coracoid muscles are then exposed with the conjoined coraco-brachialis short head of the biceps and the pectoralis minor attached to its tip. The clavipectoral fascia is divided lateral to these muscles, and a finger is passed deep to the muscles to separate them from the subscapularis (Fig. 1-10). A stay stitch is put through the proximal coracoid muscles, and extra exposure is made by dividing the lateral third of its insertion on the coracoid.
The upper and lower borders of the subscapularis are then identified. The upper border is palpated at the rotator interval, and the lower border is marked by the transverse circumflex humeral vessels. Stay sutures are then applied to the muscle belly of subscapularis approximately 2 cm from its insertion. Three stay sutures are usually all that is required.
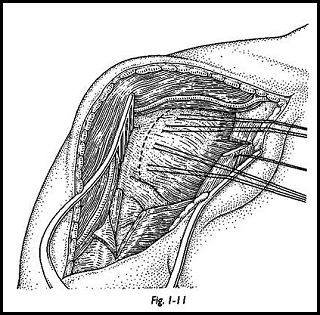
Access to the shoulder joint depends on the operation to be performed (Fig. 1-11). If this approach is used for total shoulder replacement, then the subscapularis is divided, and the joint is exposed. A skid may then be passed through the joint to lever the humeral head posteriorly so that access to the glenoid may be gained. The humeral head may be exposed by externally rotating the shoulder and dislocating the humeral head anteriorly. If the anterior exposure is being used for reconstruction and internal fixation of fractures, then the fractures at this stage can be palpated and exposed, but all muscle attachments to bone must be preserved.
Posterior Approach
The posterior approach is most commonly used for posterior stabilization surgery but also for exposure and fixation of fractures of the glenoid neck and scapula.
Position of Patient The patient is placed in the lateral position with the involved shoulder uppermost. The limb is draped free for ease of manipulation.
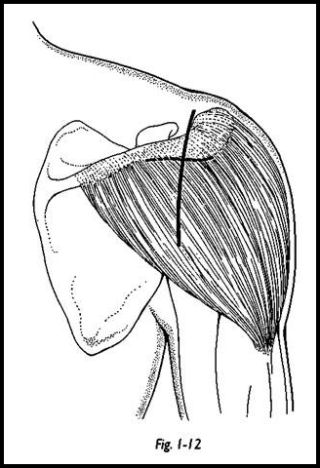
Technique A vertical incision is made in the line of the relaxed skin tension line (Fig. 1-12). The central point of this incision is the same landmark as the posterior portal for arthroscopy, that is, 2 cm inferomedially to the posterior corner of the acromion.
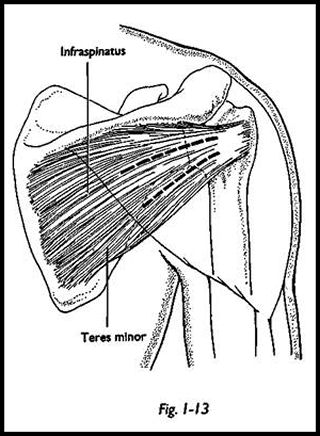
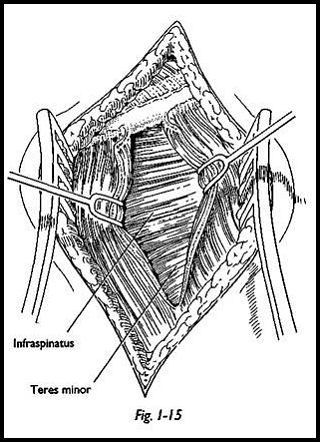
Because the skin incision does not lie in the line of fibers of the deltoid muscle, the skin is elevated medially and laterally, dissecting between the deep fascia and overlying fat. The deltoid fascia is divided, and the line of the fibers is identified. The fibers of the deltoid are separated, and the space deep to the posterior deltoid is entered through a dense layer of fascia, which is split in line with the deltoid muscle fibers. The distal limit of the deltoid split is the teres minor muscle, which will avoid damage to the axillary nerve. If any additional exposure is needed, this can be gained proximally by detaching the deltoid muscle from the scapula, taking an osteoperiosteal flap. The infraspinatus and teres minor are then exposed (Fig. 1-13).
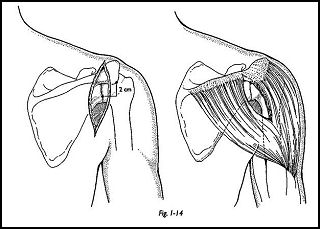
The interval between the infraspinatus and teres minor is sought but may be difficult to find; it is more easily found medially rather than laterally where the muscle fibers are conjoined. The limited dissection should be 1 cm medial to the rim of the glenoid so as not to endanger the suprascapular nerve (Fig. 1-14). Once the separation has been made and held with a self-retaining retractor, the posterior capsule of the joint can be easily seen and opened as necessary.
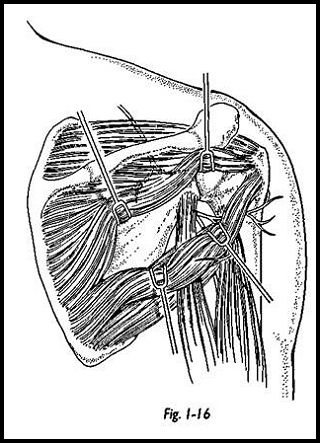
It is particularly stressed that the surgeon should try to separate the infraspinatus from the teres minor, as this allows separation between two nerve territories, that is, suprascapular nerve supplying the infraspinatus and axillary nerve supplying teres minor (Fig. 1-15). This plane, however, may be too inferior to allow the proposed procedure, and hence if infraspinatus is split, then the medial extension of this split should be limited to avoid damage to the suprascapular nerve (Fig. 1-16).
Low Anterior Approach
The low anterior approach is used for anterior and inferior stabilization procedures and can be extremely cosmetic, leaving the majority of the scar in the axillary fold.
Position of Patient The patient lies supine on the table with a sandbag under the shoulder and the arm resting on an arm board attached to the operating table with a sandbag under the shoulder as for the anterior (extended deltopectoral) approach.
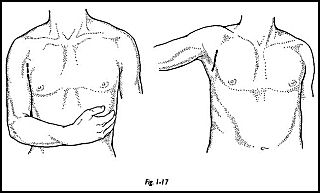
Technique The line of the incision is judged by adducting the arm across the anterior chest and noting the apex of the anterior axillary skin crease (Fig. 1-17). This lies in a vertical line from the coracoid to the apex of the axilla. The apex of the anterior axillary crease is then marked, and the arm is then abducted and extended to he on the arm board. The incision is made from this point vertically down into the axilla for 6 cm. Skin edges are undermined. The facility of this approach depends on the elasticity of the skin in this position.
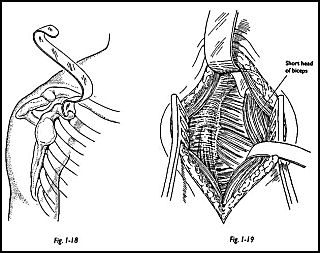
The deltopectoral junction is identified and separated by blunt dissection and held open with a self-retaining retractor. The coracoid is then palpated, and the superior angle of the wound is retracted superiorly. This is greatly facilitated by a special retractor that may be used to hook around the base of the coracoid (Copeland retractor, Ashbourne Surgical, Reading, England) (Fig. 1-18). The coracoid muscles can then be easily identified, the fascia lateral to these muscles is divided, and the lateral insertion of the coracoid muscles is partly divided (Fig. 1-19). The superior edge of the subscapularis is iden¬tified at the rotator interval, and the inferior margin is identified by the circumflex humeral vessels. The subscapularis is then tagged 'with stay sutures approximately 2 cm from its insertion, and the subscapularis is divided separate to the underlying capsule. The capsule is then opened, and the joint is exposed for whatever surgical procedure may be necessary.
Superior Strap Approach
The superior strap approach is a very useful utility approach, the anterior part of which may be used for the standard anterior open decompression procedure but when extended more posteriorly will give excellent access to the whole of the rotator cuff.
Position of Patient The patient is placed supine on the operating table in the beach chair position with a sandbag under the medial border of the scapula with the arm resting on an arm board attached to the operating table. A neurosurgical headpiece is used so that the shoulder remains free of the operating table so that both posterior and anterior access may be gained if required.
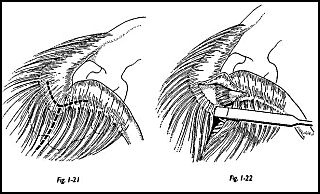
Technique A strap incision is made centered on a point half-way between the lateral border of the acromion and the acromioclavicular joint (Fig. 1-20). The skin incision is deepened through the subcutaneous tissue, and the wound is undermined by blunt dissection to expose the acromion and the acromioclavicular joint and outer end of the clavicle.
The periosteum over the acromion extending to the acromioclavicular joint is incised, and then a deep osteoperiosteal flap is raised with a small osteotome (Fig. 1-21). The purpose of this is to provide a good solid rim of tissue so that deltoid may be soundly reattached at the end of this procedure (Fig. 1-22).
.jpg)
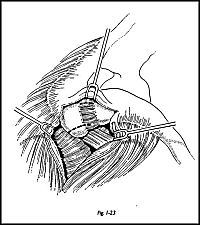
The osteoperiosteal flap is raised both on the acromial side and on the deltoid side. Anterior fibers of the deltoid are then split in the line of the fibers at the junction of the anterior third. With the middle third, there is a relatively avascular area here. The deltoid is then taken off the anterior acromion with its osteoperiosteal flap to expose the clavipectoral fascia running into a condensation of which is the coracoacromial ligament, which can be easily identified at this stage (Fig. 1-23). A self-retaining retractor is inserted, and the clavipectoral fascia may be incised to inspect the cuff. However, if this exposure is for a major repair of the rotator cuff, then anterior cuff decompression is part of this procedure and aids greatly in exposure of the cuff itself.
It is reasonable to take off the anteroinferior third of the acromion at this stage with the coracoacromial ligament. If the excision arthroplasty of the acromioclavicular joint is also required, then this may be done now. Because two thirds of the humeral head lies anterior to the anterior edge of the acromion, by careful positioning of the arm in external and internal rotation, the whole of the rotator cuff can be visualized using this exposure. If the posterior cuff needs better visualization, then more deltoid is taken off the acromion with an osteoperiosteal flap, but in the first instance, while the defect is assessed, then minimal deltoid elevation is made.
In general terms, whatever approach is used for the shoulder joint, it is always an absolute basic requirement that the deltoid must be reattached so that it may be functional immediately postsurgery. Detachment of the deltoid from the acromion and the outer end of the clavicle defunctions the shoulder and can make adequate postoperative rehabilitation impossible. Minimal detachment must be made, and if it is detached, then secure reattachment is mandatory.
Anterosuperior Approach
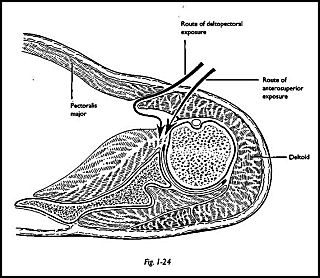
Indications The anterosuperior approach is particularly useful for total shoulder replacement, since it gives excellent face-on view of the glenoid for accurate preparation and implantation of a glenoid component. The extended deltopectoral approach is more often used for total shoulder replacement, but it can be difficult to get a satisfactory exposure of the glenoid in the well muscled. Heavy retraction of the mid part of the deltoid with consequent damage must be accepted, or partial detachment of the origins or insertion of the deltoid must be undertaken if this is to be avoided. The anterosuperior approach avoids these problems by splitting the anterior third fibers of the deltoid while also preserving the cephalic vein (Fig. 1-24). The limiting factor is the distal split of the deltoid, which must be limited to not more than 6 cm from the acromion to avoid possible damage to the axillary nerve. For this reason, it is not recommended for proximal humerus reconstructions involving displaced three- and four-part fractures and hemiarthroplasty. In these situations the deltopectoral approach affords better exposure.
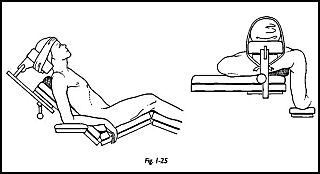
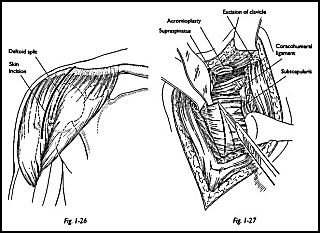
Position of Patient The patient is placed in the beach chair position with the head on a neurosurgical headpiece and the arm on a short arm board attached to the side of the operating table (Fig. 1-25). The position of the short arm board is important, since at some stage the humerus needs to be extended to allow delivery of the humeral head into the anterior wound. A sandbag is placed under the medial glenoid.
Technique The skin incision extends distally in a straight line from just posterior to the acromioclavicular joint for a distance of 9 cm (Fig. 1-26). The anterior deltoid fibers are split for a distance of not more than 6 cm, and a loose number 1 stay suture is placed in the distal end of the split to prevent further extension and possible injury to the axillary nerve. The acromial attachment of the deltoid is lifted with an osteoperiosteal flap to expose the anterior acromion and preservation of the superior acromioclavicular ligament.
An anterior acromioplasty according to the technique of Neer is performed (Fig. 1-27). If further exposure is needed, then excision of the lateral end of 1 cm of clavicle considerably enhances this.
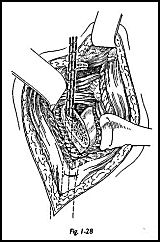
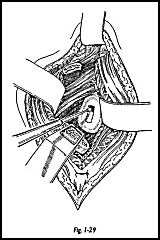
Retraction of the conjoined tendons brings subscapularis tendon into view. Subscapularis is now incised approximately 1.5 cm medial to its insertion. A Z lengthening is performed if this tendon is contracted. This is most easily performed by incising the muscles separate from the capsule; that is, the muscle is divided laterally. This in turn is swept medially, and then the capsule is divided separately just lateral to the glenoid rim. After the procedure, when repairing the subscapularis, the surgeon may attach the subscapularis tendon to the lateral capsule, hence gaining some length and allowing external rotation (Fig. 1-28). If the stemmed design of humeral replacement is to be used, the humeral head is removed, and then the medulla is prepared by extending the arm so that it is lying almost vertically (Fig. 1-29). This allows the entrance of the medullary reamers. Exposure of the glenoid is then facilitated by inserting a Fukuda ring retractor behind the posterior rim of the glenoid and a Carter Rowe spike in front, retracting the anterior soft tissues medially. The proximal humerus is depressed, and this affords satisfactory visualization of the face of the glenoid. The glenoid is then prepared in the usual way for whatever prosthesis is being used.
Transacromial Approach
Indications The transacromial approach is useful for exposure of rotator cuff and for open reduction and internal fixation of fractures of the greater tuberosity.
Position of Patient The standard beach chair position is used with sandbag under the shoulder. The patient positioned on the very edge of the operating table, and an arm board is attached to the table.
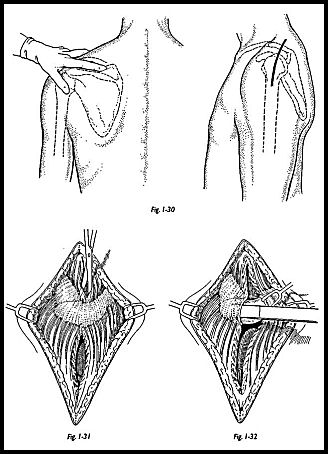
Technique The skin incision runs in the coronal plane across the middle of the acromion just posterior to the acromioclavicular joint (Fig. 1-30). The surface parking of the incision is defined by pressing the index finger into the supraspinous fossa. One side of the finger palpates the back of the clavicle while the other is in contact with the spine of the scapula. The index finger then lies in the line of the incision. The incision extends 3 cm proximally and 5 cm distal from the acromion process (Fig. 1-31).
The trapezius and deltoid muscles are split in the line of their fibers up to the acromion. Beneath the trapezius is a constant pad of fat overlying the supraspinatus, and beneath the deltoid lies the bursa, which structures conveniently define the depth of the muscles. The line of the incision across the acromion is coagulated, and an anterior and posterior osteoperiosteal flap is raised with an osteotome to allow for later closure and to maintain continuity of the trapezius and deltoid muscles (Fig. 1-32).
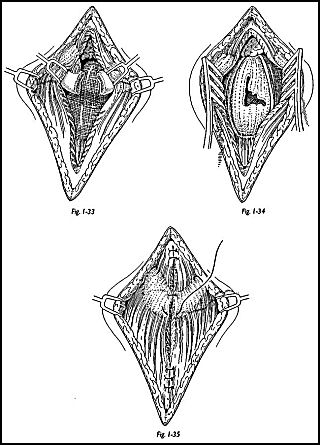
The acromion is divided with a saw or sharp osteotome (Fig. 1-33). The two halves of the acromion are retracted with a self-retaining retractor (Fig. 1-34). This then exposes the roof of the subacromial bursa, which is open to expose the rotator cuff. To allow exposure of the whole cuff, the arm is rotated externally to visualize the anterior cuff and internally to expose the posterior cuff.
On completion of the operation, the self-retaining retractor is released, and the fragments fall together and are held with a towel clip while interrupted sutures are used to close the osteoperiosteal flaps (Fig. 1-35). Providing that sound closure of the acromial flaps can be made, continuity of the trapezius and deltoid is ensured.