
Double Osteotomy
Shoulder pain that is due to pathology in the glenohumeral joint may be reheved by nondisplacement osteotomies of the neck of the scapula and the surgical neck of the humerus. Sophisticated operating theater equipment and technique are not required. The operation is of short duration, pain relief in the majority is within a day or so, and an arm sling is worn for a few days.
This procedure has been used successfully for the pain of osteoarthritis, osteonecrosis, and for both adult and juvenile rheumatoid arthritis.
History
Pain that is due to arthritis at the hip was treated by femoral osteotomy between 1935 and 1967}
Varus, valgus, and nondisplacement osteotomy in 75 percent of patients resulted in pain relief with improvement in the radiograph appearance of the subchondral bone and widening of the joint space. The mere cutting of the bone appeared to be beneficial.
From 1961, nondisplacement and displacement double osteotomy of the knee have produced a similar success rate, with the bonus that they are useful in active rheumatoid arthritis, unlike at the hip.
In 1967 double osteotomy was tried at the shoulder. Pain relief was achieved without some of the problems encountered in the lower limb, where deformity may be a major factor in these more obviously weight-bearing joints.
Indications
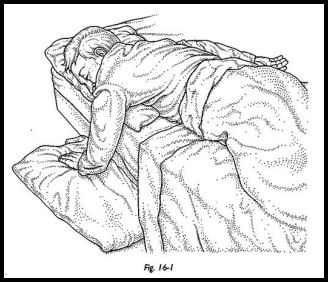
The indication for double osteotomy of the shoulder is pain in arising in the glenohumeral joint in osteoarthritis or rheumatoid arthritis. The pain must be prolonged, generally interfering with sleep and not reheved by nonsurgical measures. Loss of sleep from night pain that might tip the balance toward surgery is sometimes relieved by so simple a measure as rearrangement of pillows and hanging the limb out of bed (Fig. 16-1). Shoulder pain arising at sites other than the damaged glenohumeral joint should first be relieved.
Obvious bony damage is usually present; severe damage is not a contraindication. The elevated humeral head often reassumes its normal relation with the glenoid after double osteotomy.
Preoperative Investigation
A careful history and examination and perhaps local anesthetic injection should confirm that the source of the pain is the glenohumeral joint. Apart from this, no special preoperative preparation or blood is required.
Position of Patient
The position of the patient is critical and is supervised by the surgeon personally before scrubbing.
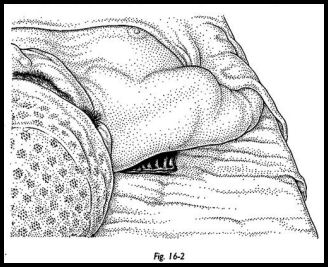
The patient lies supine, and a small bean bag is placed under the medial border of the scapula well away from the shoulder. Not a pillow, not a large bag, but a small bean bag such that the shoulder is raised by pressure on the medial scapula with no pressure beneath the shoulder joint itself (Fig. 16-2). A pillow or a bag beneath the shoulder itself fails to position the shoulder satisfactorily, and there is an unnecessary increase of bleeding.
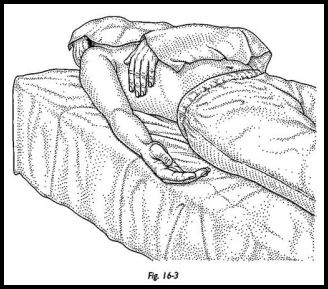
The patient is placed to the contralateral side of the table such that the ipsilateral arm lies on the table (Fig. 16-3).
It is meticulous attention to details that facilitates this operation.
Sterile towels are applied, such that the entire shoulder and the axilla, front and back, are exposed. The upper limb is toweled separately from the fingers to halfway between the elbow and the shoulder such that the upper limb can be manipulated freely during surgery.
The first assistant stands at the patient's head, the second sits or stands by the hand to control and move the arm as required.
Technique
The technique for exposing the glenohumeral joint from the front described here is based on that taught by David Trevor who had himself been taught by Bankart. The shoulder joint is accessible and apparently near the surface when approached in this way.
Anesthetic
A general anesthetic with intubation is used. The head is toweled such that the anesthetist may keep away from the patient, and there is no interference with the field of operation.
Incision
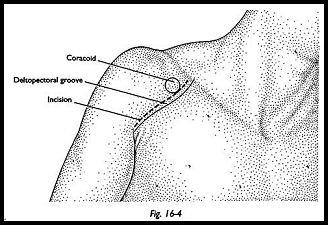
The coracoid process is palpated beneath the deltoid muscle, half an inch lateral to its medial border. The skin incision is parallel to and half an inch lateral to the deltopectoral groove (Fig. 16-4).
The deltoid is divided in line -with the skin incision XA inch lateral to the deltopectoral groove, thus avoiding the cephalic vein. If the shoulder is exposed through the deltopectoral groove, attempts to preserve the cephalic vein may end in its sacrifice. Denervation of the thin strip of deltoid by this incision causes no disability. The incision in the deltoid is in the line of the muscle fibers and can be undertaken bluntly. The clavipectoral fascia comes rapidly into view and the deltoid is retracted.
The lateral border of the tendon of the coracobrachialis and the short head of the biceps is defined and the clavipectoral fascia incised along this border from the coracoid process distally. The origin of the tendons of coracobrachialis and the short head of biceps is now mobilized. Trethowan spike retractors are placed on either side of the coracoid, and the tip with the tendon origin is removed with an osteotome. On wound closure, a flake of bone such as this probably reattaches more satisfactorily than the tendons alone.
Medial to and beneath these tendons is the brachial plexus and vessels. Dissection medial to their lateral border is avoided throughout. A small swab is placed beneath the tendons; a blunt retractor retracts medially the coracoid and its attached muscles, the end of the retractor being on the swab, which protects the plexus and vessels. Careful note of this swab is made by both the surgeon and the nurse to ensure its removal later.
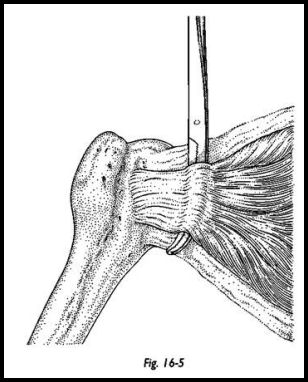
The subscapularis muscle is revealed, and the second assistant rotates the upper limb. On medial rotation, the insertion of subscapularis into the humerus is seen. From this insertion for about an inch medially, the subscapularis is fused with the capsule. The upper limb is now rotated laterally; two to three inches from the insertion, the capsule and subscapularis have separated, and it is at this site that the subscapularis will be divided. The distal extremity of the depths of the incision is now examined, and the leash of circumflex humeral vessels and nerve is seen. Just proximal to this is the distal limit of the incision into the subscapularis and later into the capsule. The closed points of a large Spencer Wells are inserted proximally in a distal direction into and beneath the subscapularis between the subscapularis and capsule emerging just proximal to the circumflex leash of vessels and nerves (Fig. 16-5).
A stay suture is inserted into the subscapularis medial to the forceps. The subscapularis is incised at right angles to its fibers by cutting down onto the forceps. The belly of the subscapularis is retracted medially with the stay suture exposing the capsule. The capsule is incised in the line of the incision into the subscapularis. Hirschowitz exposes the shoulder through a transverse incision in the subscapularis in hne with its fibers (personal communcation).
The second assistant now rotates the upper limb medially and laterally to visualize the humeral head. The Bankart skid is inserted to lever the humeral head away from the glenoid and so expose the glenoid articular surface.
Scapular Osteotomy
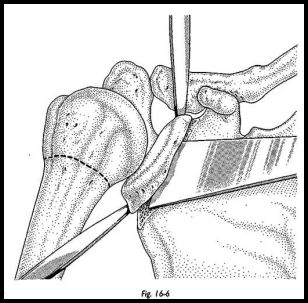
The plane of the glenoid articular surface is observed, and from this the anatomy of the neck of the scapula is visualized. Trethowan spike retractors are inserted above and below at the neck of the scapula. An osteotome, VA to 1/4-inch width, depending on the size of the scapula, is inserted at the scapula neck % inch from the joint. It is inserted parallel to the plane of the glenoid articular surface and driven across the scapula neck to just short of the posterior cortex. The osteotomy is completed by osteoclasis by angling the osteotome, moving the handle laterally, thus, separating the anterior articular surface from the adjoining scapula, thus breaking the posterior cortex (Fig. 16-6).
Humeral Osteotomy
The surgical neck of the humerus is exposed just proximal to the circumflex leash. A broad osteotome is inserted at right angles to the shaft and driven across just short of the posterior cortex.
The posterior cortex is osteoclased by angling the osteotome. Taylor and Haroon2 omit this maneuver, leaving the posterior cortex intact both at the scapula and the humerus.
The capsule and the subscapularis are sutured individually and loosely. If there is a significant internal rotation deformity, they may be left unsutured; tight suturing limits external rotation. The tip of the coracoid is reattached by coapting the clavipectoral fascia with absorbable sutures, one on either side. The small swab is removed. The rest of the wound is closed in layers. Wound drainage is inadvisable, and vacuum drainage causes undue blood loss from exposed cancellous bone and should be avoided.
The wound is dressed, and a full arm sling is applied.
This is a simple operative procedure and generally lasts less than 30 minutes from incision to application of the sling.
Postoperative Management
The patient is allowed up. The shoulder is mobilized as discomfort allows. Generally, arthritic pain is relieved immediately, and the sling is discarded within 10 days.
Results
Below are seven small series assessed simply according to relief of pain.
| Considerably Improved | |
| Shoulders | Painless or Slight Pain |
Benjamin et al.3 | 29 | 25 |
Jaffe and Learmonth4 | 32 | 29 |
Gschwend5 | 13 | 9 |
Widhalm et al.6 | 4 | 3 |
Taylor and Haroon2 | 14 | 12 |
Kelly0 | 11 | 10 |
Beacon and Hirschowitz7 | 17 | 15 |
| 120 | 103 |
The relief of pain is usually apparent within the first two postoperative days and is generally long-lasting. The first patient to undergo this osteotomy in 1967 for severe pain from rheumatoid arthritis remained free from pain in 1991.
The range of combined glenohumeral and scapulothoracic movement in the conscious patient is considerably increased. Significant increase in abduction is recorded in the majority of shoulders in which pain has been relieved. Pre- and postoperative rotation 'were measured in two series, Jaffe and Learmonth4 in 29 shoulders recorded an average gain of 25 degrees, and Kelly (personal communication, 1991) in 10 shoulders recorded gains of 20 degrees each of internal and external rotation, thus, on average gain of 40 degrees rotation. Variations in rotation gain may be due to operative technique; the capsule and subscapularis are better sutured loosely or left unsutured to avoid external rotation limitation.
Complications are few and not serious. In the author's series, one humeral nonunion occurred in an ankylosed shoulder. The patient was delighted with the increase in range of movement, which was at the pseudarthrosis. Jaffe and Learmonth4 had two humeral nonunions, 'which healed following internal fixation. Taylor and Haroon's2 method of partial osteotomy may avoid nonunion. Of Kelly's 11 cases, five did not have rotator cuffs; the condition of the rotator cuffs is not recorded in the other series. When the humeral head is elevated, it reassumes its correct relationship with the glenoid after successful osteotomy.
Conclusions
Osteotomy relieves pain and suppresses local rheumatoid activity, as is seen by the immediate postoperative regression of hot swollen synovial tissue. We do not yet know the mechanism by which this occurs. It may be the interference with large subchondral sinusoids, 'which occurs in arthritis; the division of nerves; the effect of bone healing; or some other unknown process. Double osteotomy at the shoulder is a simple inexpensive operative procedure requiring a short hospital stay. Complications are few, and the operation does not preclude a total prosthesis at a later date. In seven groups totaling 120 shoulders, 103 (86 percent) were significantly relieved of pain, and most of these had a worthwhile increase in range of movement.
References
- Nissen K: The rationale of early osteotomy for idiopathic coxarthrosis. Clin Orthop 77:98-104, 1971
- Taylor AR, Haroon M: The role of partial double osteotomy of the shoulder. Paper presented at Royal Society of Medicine, Registrars meeting, 1991
- Benjamin A, Hischowitz D, Arden GP: The treatment of arthritis of the shoulder by double osteotomy. Int Orthop (SICOT) 3:211-6, 1979
- Jaffe R, Learmonth ID: Benjamin double osteotomy for arthritis of the gleno-humeral joint, pp. 52-9. In: Rheumatology. Karger, Basel, 1989
- Gschwend N: Surgical Treatment of Rheumatoid Arthritis. Thieme 1980
- Widhalm von R, Wanivenhaus A, Markowski HP, Hackel H: Studie der Fruhergebnisse der Doppelosteotomie des Schultergelenks. Orthopadische Praxis, pp. -484—6. Sonderdruck aus Heft 6, 1982
Suggested Readings
Benjamin A: Doppelosteotomie am Schultergelenk. Orthopade 10:123, 1981
Benjamin A: Double osteotomy of the shoulder. Scand J Rheumatol 3:65, 1974
Benjamin A, Helal B: Double osteotomy of the shoulder, pp. 100-5. In: Surgical Repair and
Reconstruction in Rheumatoid Disease. Macmillan, London, 1980 Gschwend N, Kentsh A: Surgery of the Rheumatoid Shoulder, Double Osteotomy, pp. 277-8. InBateman, Welsh (eds): Surgery of the Shoulder. Mosby, London, 1984
