
Sprengel Shoulder / Undescended Scapula
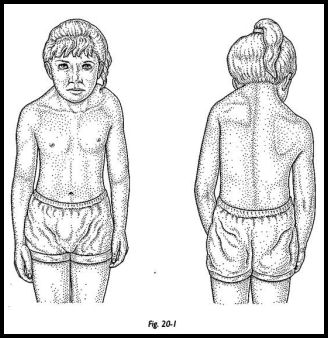
Sprengel deformity is a high shoulder blade (scapula), due to failure in early foetal development where the shoulder fails to descent properly from the neck to its final position. Normally this disorder is asymmetric with the left scapula most commonly affected, so it will sit higher on the back than the right. The condition maybe sometimes be bilateral, in which case, although it is cosmetically much more acceptable, functionally, it is more disabling. About 75% of all observed cases are girls.
Presentation
Clinically, the affected scapula usually is elevated 2-10 cm and is adducted, with it's inferior pole rotated medially. Because of this rotation, the glenoid faces inferiorly. Therefore a characteristic of the condition is a prominence in the suprascapular region because of the upwardly rotated superomedial angle of the scapula. This can cause the side of the neck to appear fuller and its normal contours to be lost.
Passive movement of the glenohumeral joint, including abduction and external and internal rotation, maybe normal, but the scapulothoracic movements may be limited.
Sometimes a bony connection is present between the elevated scapula and one of the cervical vertebra, usually C5 or C6. This connection is known as the omovertebral bone.
Treatment
Many patients with Sprengel deformity do not require operative intervention and can undergo treatments of physical therapy, which include exercises to maintain an individual's range of motion and to strengthen the weak periscapular muscles.
For those who do require surgery, it is normally undertaken in early childhood to release the scapula from what binds it to its location and then reposition the scapula and its surrounding muscles. The main objective is to improve the cosmetic appearance and contour of the neck and to improve the scapular function. The optimal age for operative intervention is generally agreed to be younger than 8 years old. Surgical treatment in adulthood is almost impossible and complicated by the risk of nerve damage when removing the omovertebral bone and when stretching the muscle tissue during relocation of the shoulder.
Surgery
There are multiple surgical procedures for this Sprengel Shoulder.
1. Scapula Osteotomy 2. Green's Procedure 3. Woodward Procedure The supraspinous portion of the scapula is
resected with its periosteum. Care is taken to avoid injury to the
suprascapular nerve and vessels. The scapula is then lowered to the
desired position. The subscapularis muscle is reattached to the
vertebral border, and the supraspinatus is sutured to the scapular
spine. The serratus anterior is reattached to the vertebral border, and
the latissimus dorsi is reattached to the scapula. The trapezius and the
rhomboid muscles are then resutured to the spinous processes at a more
distal level. The wound is then closed in layers.
In the Green’s procedure,
muscles are detached from their scapular insertion, the trapezius
muscle is then elevated extraperiosteally and reflected medially, thus
exposing underlying muscles and the scapula. The supraspinatus muscle is
then detached from the scapula along with its periosteum. The
omovertebral bone, when present, is excised. The insertions of the
levator scapulae muscles on the superior angle of the scapula and of the
rhomboid muscles on the medial border of the scapula are dissected. The
supraspinous fossa of the scapula is resected, taking care to avoid
injury to the suprascapular neurovascular bundle. The scapular
attachments of the latissimus dorsi and serratus anterior muscles are
detached from the anterior aspect of the scapula. The scapula is then
displaced distally down to the level of the normal side using the
superiomedial angle of the scapula as a landmark rather than its tip
because of constant scapular hypoplasy. Once the scapula is in its
corrected position, the muscles are reattached to it, the supraspinatus
muscle to the base of the scapular spine, rhomboid muscles should be
reinserted without compromising the new position of the scapula in the
frontal plane by lengthening it if necessary, in order to achieve good
orientation of the glenoid and therefore increase in the range of
abduction. Some modifications were brought to the initial Green’s
procedure: a clavicular osteotomy is performed first to reduce the risk
of brachial plexus palsy (BPP); the insertion of the serratus anterior
is dissected from the spinal border of the scapula and scapula adherence
to the thoracic wall is separated; insertion of the supraspinatus
muscle is resected, the inferior pole of the scapula is sutured to the
thoracic cage into a pocket of the latissimus dorsi muscle. (Green W.T. The surgical correction of congenital elevation of the scapula (Sprengel's deformity) J Bone Joint Surg Am 1957; 39-A: 1439-1448) (Andrault G., Salmeron F., Laville J.M. Green's surgical procedure in Sprengel's deformity: Cosmetic and functional results Orthopaedics & Traumatology: Surgery & Research 2009; Vol 95, no 5: 330-335)
In the Woodward procedure, the patient is placed in the prone position. A midline incision is
made from C1 to T9. The wound is dissected laterally to the medial
border of the scapula. The lateral border of the trapezius is
identified. The lower portion of the trapezius is dissected from the
latissimus dorsi muscle. The origin of the trapezius is detached from
the scapular spine, and the edges are tagged. The origins of the
rhomboid muscles are divided and tagged. The entire muscle sheet is
retracted laterally, exposing the omovertebral bar, which is excised
extraperiosteally. The levator scapula muscle is sectioned at its
attachment to the scapula. Fibrous bands may attach the scapula to the
chest wall; these should be sectioned. The serratus anterior muscle must
be detached from its insertion in the vertebral border of the scapula.
The supraspinatus and the subscapularis muscles are elevated
extraperiosteally.
A new modified method of this procedure also involves a osteotomy or morcellation of the middle one third of the clavicle to avoid compression of neurovascular structures at the thoracic outlet. (Carson W.G., Lovell W.W., Whitesides T.E. Congenital Elevation of the Scapular, surgical correction by the Woodward procedure. J Bone Joint Surg Am 1981; 61-A: 1199-1207)
