
Scapula fixation
Disorders such as facioscapulohumeral dystrophy (FSHD), neuralgic amoyotrophy, long thoracic nerve palsy, spinal accessory nerve palsy and dorsal scapular nerve palsy, which affect the muscles that attach to the scapula that coordinate scapulothoracic motion can result in winging of the scapula and subsequent scapular dyskinesis.
The images below document surgery for scapula fixation
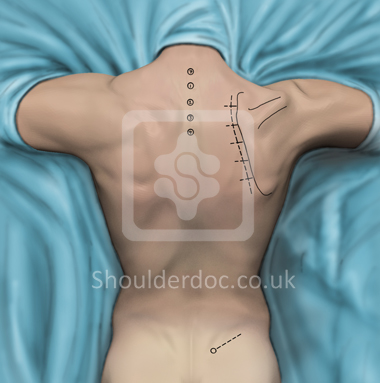
The patient is placed prone on a Wilson spine table. The arm on the operative side is placed in approximately 90 degrees of abduction and external rotation. Bony landmarks, such as the superior, medial and inferior borders of the scapula, the scapular spine and the spinous processes of the seventh cervical and first four thoracic vertebrae along with their associated ribs are identified and marked with pen. The spine of the scapula should overlie the fourth rib.
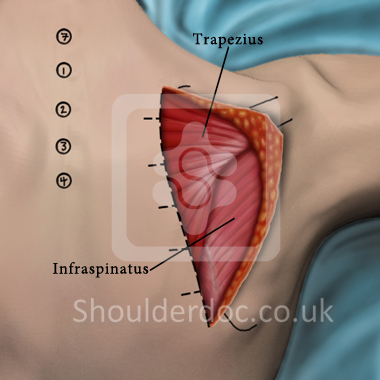
An incision is made along the medial border of the scapula through the skin and subcutaneous tissue. The dorsal surface of the trapezius muscles that overlies the scapula is exposed.
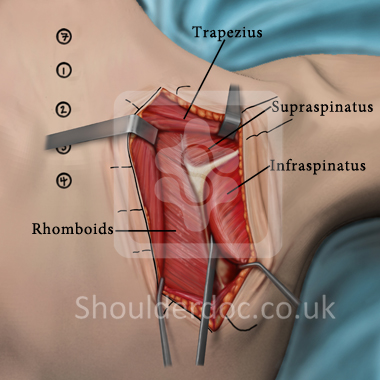
Trapezius is lifted from the lateral aspect of the spine of the scapula to expose supraspinatus and infraspinatus. A Cobb elevator is used to elevate supraspinatus and infraspinatus from the underlying scapula. Once the medial 3cm of the scapula are exposed, a towel clip is placed
around the scapula spine to elevate the scapula and place the rhomboids
under tension on the medial scapular border. The rhomboids are then
detached and the subscapularis is elevated from the ventral scapular
body, exposing the medial 6cm of the scapular body.
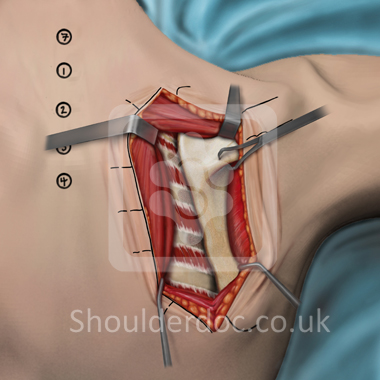
An incision is made through the raphe between the rhomboids and serratus posterior to expose the subscapularis bursa. Using the seventh cervical spinous process as a landmark, the third, fourth, fifth and sixth ribs are exposed.
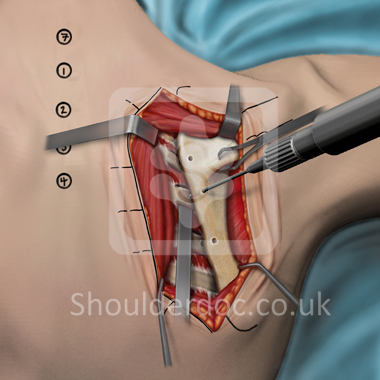
Careful subperiosteal dissection of the ribs is performed to separate the ribs inferiorly and superiorly from the intercostal muscles and ventrally from the parietal pleura of the lungs. The exposed ribs and ventral surface of the scapula are lightly decorticated with a high speed burr. A malleable retractor is passed carefully under the ribs to protect the lungs when a burr is used to place holes in the scapula and ribs. A single hole is placed in the supraspinatus fossa directly over the third rib. Two drill holes each are placed through the exposed scapular body over the fourth and fifth ribs. Bone graft is obtained from the posterior superior iliac spine of the pelvis and is placed between the third, fourth, and fifth ribs under the exposed medial scapula.
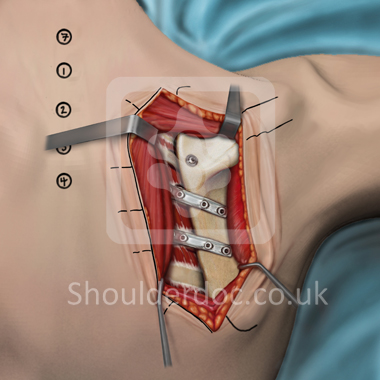
The scapula is then positioned such that the angle formed by the spinous
process and the medial border of the scapula measures 20-30 degrees and
the inferiomedial pole of the scapula is approximately 5-7 cm lateral
to the spinous processes. Then finally two contoured plates are placed
in the infraspinatus fossa and a single screw placed in the hole in the
supraspinatus fossa, which are screwed into place through the scapula
and underlying ribs thus insuring a tight fit between the scapula and
ribs.
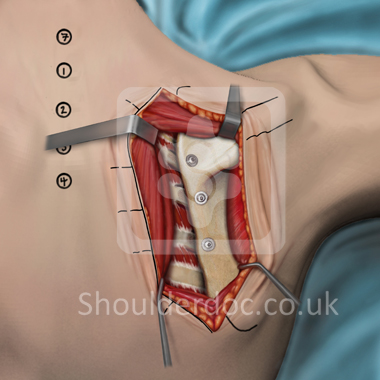
Alternatives include just screws instead of the plate and screw method
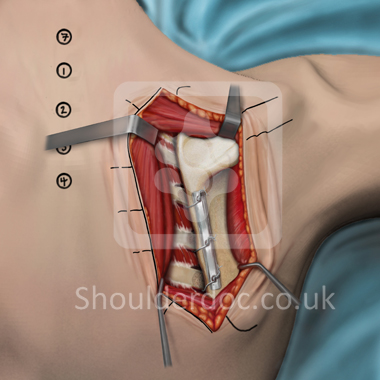
Or the plate and wire method.
Once the scapula is fixed to the underlying ribs, the elevated supraspinatus and infraspinatus are allowed to fall back to their original positions, providing soft tissue coverage over the hardware. The rotator cuff musculature and scapular stabilizers are then re-approximated to the medial border of the scapula. The wound is then closed in layers and a dressing applied. The arm is finally placed in a sling.
