
Introducing the needle
A needle is then introduced from the posterior portal entry site, aimed at the surgeon's finger, which has been placed on the coracoid process (Figure 4.18). At this point, it is of benefit to ask for silence in the operating theatre. The assistant then distracts the arm towards the patient's feet, and resistance is felt as the posterior capsule is encountered, followed by a sucking sound as the joint is entered. If there is an effusion within the joint fluid may then escape from the needle showing correct placement (Figure 4.19), but this is rare.
.jpg)
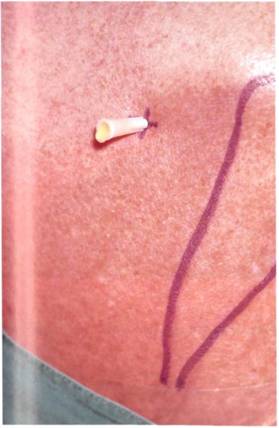
Figure 4.18 A needle is inserted from the posterior portal aimed at the coracoid process.
Figure 4.19 A sucking noise is heard as the needle enters the joint. If there is an effusion (which is rare) joint fluid may exit from the needle.
A 50 ml syringe is connected to the needle and the joint is prefilled with irrigating fluid (Figure 4.20). We have found that the shoulder will take over 40 ml on average, and up to 70 ml in dislocating shoulders. Free backflow of fluid into the syringe shows correct placement of the needle inside the glenohumeral joint. If there is no backflow, then the needle should be removed and replaced in a better position.
Difficulty can be encountered in prefilling the joint for one of several reasons. The first is inexperience which, of course, is unavoidable. The second is through obliteration of the landmarks by obesity or muscle. A longer needle (spinal needle) is needed. The third reason may be rotator cuff tears, which allow the fluid to pass straight out of the joint into the subacromial space. The last reason is in the stiff painful joint, where the joint is obliterated by synovitis.


Figure 4.20 The joint is prefilled with sterile irrigation solution. Free backflow shows correct placement.
Figure 4.21 An incision along the Langer's line is made at the portal site.
The needle and syringe are removed following prefilling. The skin is then punctured using a No 11 surgical blade at the portal site. The incision should follow Langer's lines, and should be long enough to allow the insertion of the arthroscope (Figure 4.21). The sharp trochar and cannula are inserted, following the needle track and aiming for the finger on the coracoid process (Figure 4.22). Fluid is seen to escape from the open side tap showing correct placement (Figure 4.23). The arthroscope is inserted in the place of the trochar, and connected to the irrigation fluid and to the light source (Figure 4.24). The arthroscopic camera is then connected (Figure 4.25), and the camera and light source switched on.


Figure 4.22 The sharp trochar and cannula are then placed following the line of the withdrawn needle.
Figure 4.23 Fluid escape from the prefilled joint shows successful placement.
A needle is placed via the anterior portal, the surface marking of which is halfway between the coracoid process and the anterior edge of the acromion, pointing directly towards the arthroscope (Figure 4.26). Entry is confirmed by the outflow of irrigation solution (Figure 4.27). This ensures a free movement of fluid which keeps the joint clear of blood. The difference in calibre of the entry and exit cannulae ensures that pressure is maintained within the joint, as well as establishing a flow.

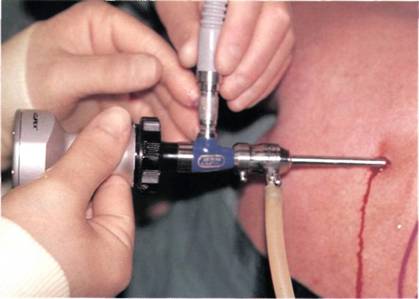
Figure 4.24 The arthroscope is inserted in the cannula, and irrigating fluid and light cable attached.
Figure 4.25 The arthroscope camera is finally attached.
After the joint has been examined visually (see Chapter 5), extra information is gleaned by palpation. A hook probe needs to be passed from the anterior portal (Figure 4.28). Instruments can be placed into the joint through the anterior portal freehand or through a cannula.
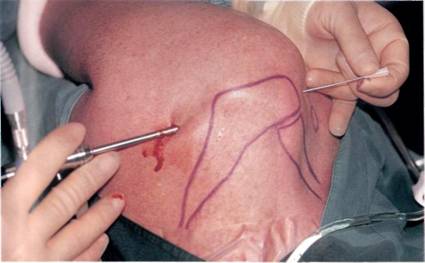
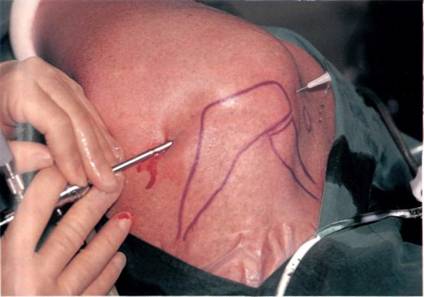
Figure 4.26 A needle is then placed from the anterior portal pointing towards the arthroscope.
Figure 4.27 Escape of irrigation fluid shows successful placement of the needle, which ensures free flow of fluid and keeps the joint clear of blood.
