
Bursal endoscopy
After the glenohumeral endoscopy has been performed, it is essential to pass on to the bursal side examination. The arthroscope cannula and sharp trochar are passed either through the same posterior skin incision, or through a separate and slightly higher (cephalad) stab. The sharp trochar is exchanged for the blunt trochar and pushed forward under the acromion until the end of the trochar rests on the coracoacromial ligament. This is helped by the assistant pulling the arm downwards (caudad) with the arm to the side.
The most common error in bursal endoscopy is to fail to enter the bursa, and the reason for this is simply that most surgeons believe that the subacromial bursa lies under the acromion. In fact it can consistently be entered under the coracoacromial ligament but its extension under the acromion is variable. Bayley (personal communication, 1989) has classified the bursa into three types: where the bursa extends under the anterior one-third of the acromion; where its posterior limit is the anterior edge of the acromion; and where it extends under the anterior two-thirds of the acromion.
In order to enter the bursa every time, therefore, the trochar must be inserted until it is anterior to the acromion and the free lateral edge of the coracoacromial ligament can be flicked on the end of the trochar. The trochar is now withdrawn and the arthroscope inserted. If a large cavity is seen (Figure 4.32), then irrigation may be switched on to expand the bursa. If all that is seen is cobwebs (Figure 4.33), then the bursa has not yet been entered, usually because the cannula is not far enough forward. The irrigation should not be switched on, as this will make entry more difficult. The process is repeated with the cannula further forward.
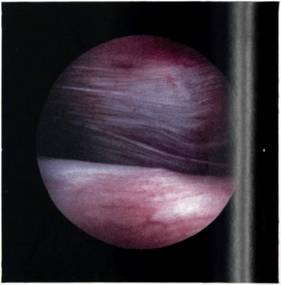
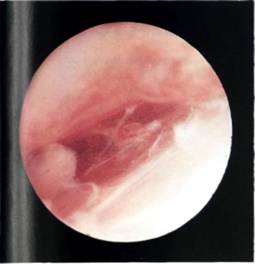
Figure 4.32 If the bursa has successfully been entered, then a large cavity is seen.
Figure 4.33 If the bursa has not been entered, then the arthroscope is in the subacromial areolar tissue and a 'cobweb' appearance will be seen.
Orientation within the bursa is more difficult as there are no helpful landmarks like the long head of biceps. It is therefore helpful at this point to insert two needles, one at the anterolateral edge of the acromion and one at the acromioclavicular joint.
Operative portals for subacromial decompression are described in Chapter 8.
