
Index
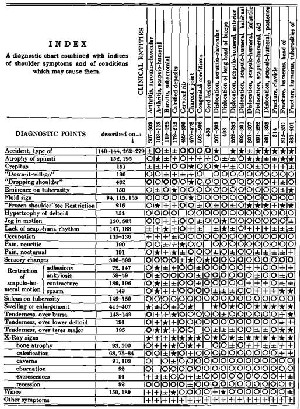
THE USE OF THE INDEX CHART
The numbers below the diagnoses refer to the pages where the lesions are described; those in the vertical column, next to the list of diagnostic points, refer to the pages on which these points are explained. Thus the student, when using the chart, may readily obtain more information about dubious points.
To use the chart to summarize the symptom-complex of any clinical entity, make separate lists of diagnostic points for each form or symbol in the vertical column under that entity, then write after each list as follows:
* (list) "are of positive importance in this diagnosis."
+ (list) "are of positive importance, but not in all stages or in all cases."
± (list) "are sometimes present but are often absent."
O (list) "the presence of these would be contradictory to this diagnosis,
so that their absence is important."
O (list) "are usually not present, but their presence is not important."
Square (list) "the author has no opinion."
For instance, in complete rupture of the supraspinatus:
* The type of accident, atrophy of spinati, crepitus, eminence on tuberosity, fluid sign, jog in motion, lack of scapulo-humeral rhythm, occupation, nocturnal pain, restriction from spasm, sulcus on tuberosity, tenderness over bursa and over teres major, bone atrophy, wince—are of positive importance in this diagnosis.
+ "Down-it-will-go," hypertrophy of deltoid, tenderness over lower deltoid, the X-ray signs of caverns, eburnation, excrescences, recession and other symptoms—are of positive importance, but not in all stages or in all cases.
± Dropping shoulder and neuritic pain—are sometimes present but are often absent.
O Frozen shoulder, sensory changes, restriction from adhesions, ankylosis or contracture; swelling or enlargement, calcification—the presence of these would be contradictory to this diagnosis, so that their absence is important.
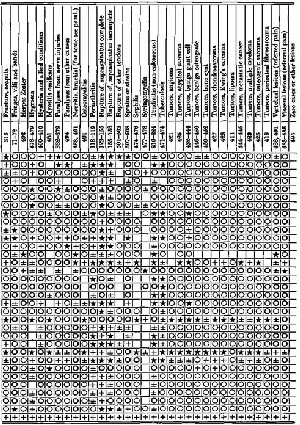
To use the chart to find the clinical entities which any one symptom may indicate, follow the transverse column, making separate lists of the diagnoses above each kind of symbol. Combine these lists as before with the same sentences, using the singular instead of the plural, and vice versa, thus:
* A jog in motion—is of positive importance in these diagnoses—dislocation of the long head of the biceps, fringes, villi and bands, complete rupture of the supraspinatus tendon.
+ A jog in motion—is of positive importance, but not in all stages or in all cases of—subacromial bursitis, calcified deposits, incomplete rupture of the supraspinatus, benign giant cell tumor.
± A jog in motion—is sometimes present but is often absent in—congenital conditions, fracture of the tuberosity, fracture of the scapula.
O A jog in motion—the presence of this would be contradictory to these diagnoses, so that its absence is important—cervical rib, herpes zoster, hysteria and allied conditions, neuritis, periarthritis, sprains or strains, tendinitis, tuberculosis, vertebral lesions, visceral lesions.
O A jog in motion—is usually not present but its presence is not important in—acromioclavicular arthritis, scapulo-humeral arthritis, Charcot's joint, cord lesions, dislocations, hygroma, myositis ossificans, paralysis, osteomyelitis, etc.
The chart is capable of presenting a whole chapter on differential diagnosis, as the reader may prove, by writing out after this fashion the information contained in all the vertical and transverse columns.
The last transverse column shows none but -f- marks, indicating that there are other symptoms not typical of shoulder lesions but which help to clinch the diagnosis, such as the lead line in "paralysis, other forms," dissociated anaesthesia in syringomyelia, ecchymosis in the various fractures, the blood conditions in syphilis, tuberculosis, osteomyelitis, etc.
The last vertical column leaves room for the addition of new diseases, or of some of the rare ones briefly mentioned in the text.
There are of course many imperfections. For instance, the list of entities should not contain synonyms or terms partly synonymous, such as "tendinitis" and "periarthritis." Nor, in my opinion, should it contain "brachial neuritis." I have dared to leave out "rheumatism" and "neuralgia," but the believers in an idiopathic "neuritis" are too numerous to ignore. Its only symptom or sign is pain along the nerve trunks, and this symptom is a very common one in other conditions which can readily be relieved by treatment on the bases of other diagnoses!
Unsatisfactory as this list may be, I challenge any student or professor to produce a better one, for our science, as yet, is too imperfect. Who can make a list of the diseases of this or of any other part of the body without having the nightmare of symptoms appearing as diseases called by shifting, unstable synonyms? At any rate, it offers a form of mental exercise for any one who may be interested in lesions in and about the subacromial bursa.
