
Rupture of the supraspinatus tendon
CHAPTER V
Now that we have considered the shoulder from the anatomic and pathologic points of view, we come to the clinical study of the lesions which may be identified by special groups of symptoms as definite entities. It seems to me that the practice of medicine might be greatly simplified if an official list of clinical entities was constantly maintained by some great medical association. Our literature and our methods of medical education are greatly hampered by synonyms. McCarthy has recently pointed out in Surg. Gyn. and Obst., February, 1932, that there is great need for such a list of malignant conditions. Pathologic entities and clinical entities are not the same. Clinical entities are the practical working diagnoses on which rational treatment may be based. I feel that the Registry of Bone Sarcoma has served such a purpose so far as the nomenclature of bone tumors is concerned, and that this fact alone has done much to crystallize our working knowledge of the diagnoses and treatment of bone lesions.
I shall try in this book to make a. similar list of the lesions of the shoulder which have such distinctive characters that they may be recognized clinically and given appropriate treatment. For instance, I recognize as significant clinical entities, complete rupture of the supraspinatus tendon, partial rupture of the supraspinatus tendon, calcified deposits in the tendons of the short rotators, and tendinitis of the short rotators; and I do not recognize muscular rheumatism, neuritis, or idiopathic monarticular arthritis of the shoulder, as entities of sufficient clinical frequency or importance to make them demand special forms of treatment, although these terms are much more frequently used as diagnoses on which physicians base their therapeutics. If an official list existed I would ask to have my new entities added and the old ones at least put in small type. The reader is referred to the Index.
.jpg)
CHART I
Excluding obvious diagnoses such as tumors, fractures and dislocations, most painful shoulders may be classed under the four diagnoses indicated in large type, although each entity merges into the two which adjoin it. For example, calcified deposits are probably a product of tendinitis, but if large in amount, they alter the clinical picture, both in prognosis and in the character of treatment required. If the deposits are very small, they may be negligible, and the clinical picture be that of a "frozen shoulder" due to tendinitis, lendinitis may also be confused with its other neighbor, because a "rim rent" may precipitate the inflammation which results in the frozen shoulder. In a similar way the line between partial and complete ruptures is difficult to draw; e.g., some cases of partial ruptures do not show much restriction of motion. Even complete ruptures may be confused with calcified deposits, as in Case 76, where the tendon was torn through a partially calcified area. Pathologically, too, there is some reason to believe that calcified deposits may be caused originally by small ruptures, and that the defects left after the deposits have disappeared may later lead to rupture. Nevertheless, although these entities are difficult to separate in borderline cases, typical instances are very clearly distinguished for purposes of treatment as well as in prognosis. There are also suggestive variations in sex, age, and occupation among the patients subject to these conditions.
This chapter discusses the most serious of these entities. As far as I know, I was the first writer to call attention to this lesion, and it seems to me that I can best introduce the rest of the book by reprinting here my first article, so that we may thus start at the beginning, so far as the history of this particular entity is concerned.
----------------------------------------------------
Reprinted from the Boston Medical and Surgical Journal, Vol. clxiv, No. 20, pp. 708-710, May 18, 1911
COMPLETE RUPTURE OF THE SUPRASPINATUS TENDON. OPERATIVE TREATMENT WITH REPORT OF TWO SUCCESSFUL CASES
In a paper on "Stiff and Painful Shoulders," published in the Boston Medical and Surgical Journal for May 31, 1906, in speaking of rupture of the supraspinatus tendon in connection with subacromial bursitis, I presupposed, on anatomic grounds, the probable symptoms of such rupture as follows:
"One theoretical symptom (since the supraspinatus is put out of action) should be the persistence of passive and loss of active abduction. I am not ready to say this as yet, however, because in most cases the pain is so great that spasm prevents even passive motion, and later adhesion takes the place of spasm. When rupture of the tendon does take place, it probably is only partial and a Y-shaped attachment still remains to perform part of the function. In a similar way, the quadriceps may extend the femur when the patella is broken if the lateral expansions of its tendon are not torn. Nevertheless, I believe that the active function of the supraspinatus is important in elevation of the arm."
Since this paragraph was written I have had two cases of complete rupture of the supraspinatus tendon on which I have operated, and in both of which I was able not only to demonstrate the existence of the anatomical lesion in conjunction with the above symptoms, but succeeded by suturing the tendon to the tuberosity in bringing about complete restoration of the function of abduction. I have also, in a number of cases, verified the clinical diagnosis of a partial rupture such as depicted in the accompanying figure, which was produced in the other articles which I have written on this subject. (The reader is referred to the articles appearing in the Boston Medical and Surgical Journal for Oct. 22 and 29, Nov. 5,12,19 and 26, and Dec. 3, 1908. The figure alluded to is not repeated here.)
This partial rupture is the common lesion, and, as I have explained, the remaining portion of the tendon is competent to take up the function when the sensitiveness due to the reparative process about the point of rupture has disappeared. The curious deposits of lime salts sometimes shown in the X-ray, and spoken of by Painter and Baer, are, I believe, faulty attempts at repair of these tiny ruptures of the tendon.
The following two cases are quite definite because they present complete rupture of the tendon of the supraspinatus. Therefore, the function of active abduction was almost entirely lost.
CASE 1.—Mrs. J. A. Aged fifty-two. Born in Scotland. Referred by Dr. Kent, of Dorchester, March 7, 1909.
Patient had always been a healthy, hard-working woman and had practically never been sick. On Oct. 3 of the previous year, i.e., five months before I saw her, while she was hanging recently washed clothes on the line in her yard, she endeavored to toss over a heavy blanket and felt something snap in her shoulder as she threw her arm up. She felt an intense pain and her arm fell and "hung by her side for a while." She was examined later by Dr. Kent, who found no thickening or ecchymosis. An X-ray was negative. Since then she had not been able to abduct the arm and had suffered much pain at night and somewhat during the day. The symptoms were in general those which I have described as the symptoms of adherent subacromial bursitis. The following points were, however, noticeably different.
(1) There was little atrophy of the deltoid, and it even appeared hypertrophied on account of the apparent swelling of the joint beneath. (2) Under the fibers of the deltoid, beneath the acromion and over the joint, there was a distinct deep fluctuation as if the whole bursa were full of fluid. (3) The ability to start abduction was absent, but when the arm was passively abducted to about 140°, the patient, by a strong contraction of the deltoid, could prevent the arm from falling for an instant, but the slightest downward pressure made it drop to the side. External rotation was about one-half the normal.
Operation.—March 11, 1909. Usual incision between fibers of deltoid. Roof of bursa abnormally thick with granulation-like bodies on its under surface. Escape of straw-colored fluid, about one-half ounce. The floor of the bursa was found communicating with the joint, because practically the whole supraspinatus was torn from its insertion and retracted inwards. The biceps tendon was exposed over the articular surface, but was apparently uninjured. For about one-half inch on the lower visible portion it was bright pink; the rest of it was normal in appearance. By holding the bursa wide open,
pulling down on the arm and raising the elbow from the table, the retracted end of the supraspinatus could be seen. This was caught with a tenaculum and pulled down enough to suture with four heavy silk threads to the remaining portion still attached to the tuberosity. This could not be done exactly, but was done nearly enough so that it seemed possible for repair to take place along the silk sutures. A little gap was also left on each side, which was not covered with tendon substances. It was in a sense a suture a-distance. When the operation was completed it seemed as if there was a fair possibility of the supraspinatus obtaining enough attachment to enable it to perform its function, although the base of the bursa would necessarily remain a rough instead of a smooth surface. Dr. Kent gave ether, Dr. Vincent assisting. Dr. J. J. Putnam and Dr. M. P. Smith-wick present.
June 9, 1909. Looks very strong and well. Sleeps well. Arm aches at times but not much. Pain in stormy weather (after use). Gets good use out of arm and does her own work. Can button back of dress and do her own hair. Real free abduction to 135°. Fair rotation. Muscles developing well and deltoid is strong. Very much pleased with result.
This patient was demonstrated to the Interurban Orthopedic Club, March 25, 1911. The arm is perfectly well and the function is perfect. The only abnormal sign is that the deltoid is unusually prominent due to the presence of joint fluid in the bursa.
CASE 2.—Mr. D. R. Aged forty. Hostler. Referred by Dr. John Homans, Dec. 21, 1910.
Patient is a strong, wiry Irishman. He has always been well. About three and one-half months previously, he had been saddling a horse in the stable and while tightening the girth he felt something in his shoulder give way and he fell to the floor. There was immediate loss of power in the arm, but lie managed to finish saddling the horse without raising that arm. That night he consulted Dr. Luce, of Canton, who found no ccchymosis, but thought there was slight crepitus. An X-ray a little later was negative. The hip was also hurt by his fall, so that for some time he was more bothered by that than he was by his shoulder and he was obliged to use crutches for several weeks. At the time he presented himself to me for examination the symptoms were at first sight those of the adherent type of subacromial bursitis, but on more careful examination the same signs that were present in the previous case were demonstrable, that is, (1) Relatively slight atrophy of the deltoid and an appearance of hypertrophy. (2) Fluctuation over the region of the bursa beneath the deltoid producing a "verwblbung" of the latter. (3) The persistence of nearly normal passive abduction with no active abduction. When the arm was passively abducted, the patient by a strenuous exertion of the deltoid could hold the head of the bone on the glenoid and thus prevent the arm from falling immediately. (4) In this case a distinct depression could be felt just above the tuberosity at the point where the tendon was torn away from the latter. A definite diagnosis was made and the members of the Boston Orthopedic Club invited to examine the case and witness the operation.
Operation.—Jan. 10, 1911, at the Massachusetts General Hospital.
As in the previous case, when the fibers of the deltoid.and the thickened roof of the bursa were incised, there was an escape of straw-colored fluid and the bursa was found to be in communication with the true joint. The supraspinatus had retracted so far that at first it could not be seen, and one looked directly at the articular surface of the bone with the uninjured biceps tendon lying across it. With some difficulty the supraspinatus tendon was caught with a tenaculum, freed and pulled forward. It was then sutured "a-dis-tance" to the tuberosity with heavy silk prepared with paraffine after the manner of Lange. As in the previous case, the retracted tendon could not be entirely united, but enough strands of silk were put in to make it possible for the function of the tendon to be replaced.
Convalescence was normal and the patient was not allowed to use the arm in abduction for three weeks, but since then has been using it with more or less freedom. He was shown to the Interurban Orthopedic Club on March 25, and the following condition noted at that time:
Patient is working every day—can chop wood and do other "chores" without pain. He can easily place his hand on top of his head or behind his back. Full abduction of the humerus on the scapula is, however, weak, and although he can elevate his arm, he cannot hold it in an abducted position against a downward pull of even moderate force. The strength of the arm in other respects is excellent and the patient is well satisfied. The function of the supraspinatus is fully as good as it was in Case 1, at the same length of time after the operation.
I have seen only one other case in which I have made a diagnosis of complete rupture of the supraspinatus, and as I have not been able to persuade this patient to allow me to operate, his present condition is very instructive as compared to the two cases mentioned above.
In spite of the fact that the patient is a powerful man with an extremely well-developed deltoid, he is now, four years after the injury, still unable to start abduction. As in the other cases, however, when the arm is passively abducted so that the patient's deltoid acts in the same line of force as the axis of the humerus and the remaining short rotators {i.e., subscapularis, teres minor, infraspinatus), the head of the humerus obtains a fairly firm contact with the glenoid so that the weight of the arm can be held by a great effort of will on the part of the patient. The slightest pull downward on the arm, however, will overcome what little power he has, and as soon as the fulcrum on the glenoid is lost, the arm drops to the side.
It will be necessary for those readers who are interested in this subj ect to refer to the articles mentioned above to thoroughly understand this one, but, best of all, they should look for themselves at dissecting-room subjects, because injuries to this tendon are so common that I have never had any difficulty in finding examples of it in a single set (20) of dissecting-room subjects.
The injury, as I have explained, is usually confined to a partial rupture of not more than one-quarter to one-half inch in breadth. Such complete cases as these three which I have reported are exceptional. The smaller ruptures, which are not of sufficient mechanical importance to interfere greatly with the function of the arm, are best considered with the subacromial bursitis which they cause. It must be understood that these ruptures are beneath the serous base of the bursa, which may or may not be torn through. If it is torn through, a communication is established between the bursa and the true joint.
In operating for subacromial bursitis, if on entering the bursa one finds straw-colored joint fluid, a careful search will usually demonstrate a small opening into the true joint at the point of rupture. In only one case has it seemed worth while to me to make an attempt to suture one of these small ruptures. Usually these heal satisfactorily if the inflamed portion of the bursa over them is clipped away with scissors. I am convinced, nevertheless, that suture is necessary in long-standing complete cases such as those cited above. The one which was not sutured has a decidedly impaired function and for two years was unable to work.
I have never seen the tendons of the other short rotators ruptured except in conjunction with that of the supraspinatus. Twice I have seen a longitudinal split between the tendon of the subscapularis and that of the supraspinatus. (End of 1911 paper.)
.jpg)
FIGURE 38. RUPTURE OF THE SUBSCAPULARIS
Sketch by Mr. Aitkin of a specimen found and prepared in the dissecting room by my former assistant, Dr. T. W. Stevenson. It illustrates a rupture of the subscapulars without rupture of the supraspinatus, and is instructive from several points of view. This is the only instance of an exception to the statement in the last paragraph which has come to my knowledge in the twenty-two intervening years. It gives a very good idea of how the insertion of the supraspinatus, which in this specimen was intact, normally fills the sulcus at the anatomic neck, and covers the tuberosity, thus leaving a perfectly smooth exterior contour beneath the base of the bursa. In this case the bursa has been thoroughly dissected away in order to show the superficial fibers of the tendons passing over the tuberosity and becoming continuous with the periosteum below. In Chapter X it will be shown how these fibers cover up and hold together the fragments in comminuted fractures.
The figure also gives a good idea of the manner in which the supraspinatus emerges from under the coraco-acromial ligament and acromion. The lower or inner edge of the muscle has been rather sharply dissected, but in the undissected specimen this edge blended with the upper portion of the subscapularis. Below this, one sees that most of the subscapularis has been torn away from the conjoined tendinous cuff, so that the biceps tendon, running through its groove between the two tuberosities, is exposed at the left edge of the gap. Internal to the biceps tendon we see the lesser tuberosity, from most of which the subscapularis fibers have been evulsed. The knobby character of the surface of the exposed tuberosity is shown; an appearance usually found in old cases where the tuberosity is exposed by evulsion of the fibers of any of the other tendons. (See frontispiece and Fig. 40.) In other words, this knobby look is the superficial appearance of the "excrescences" or "volcanoes" spoken of on page 91, and also shown in Plate V, Fig. 1.
In the upper half of the gap above the excrescences is the exposed cartilage of the joint. If this gap extended outward from the biceps tendon, instead of inward, it would represent the condition which we usually see; i.e., rupture of the supraspinatus rather than of the subscapularis. It is not unusual to find in the dissecting room extensive tears involving both tendons, but it is very unusual to find the subscapularis involved alone, as in this case. One can readily picture how easy it would be to produce such a condition as this by forcibly performing external rotation in a case of "frozen shoulder."
This diagram also gives an excellent idea of the coracoid process, coraco-clavicular and coraco-acromial ligaments, as well as of the conjoined origin of the internal or short head of the biceps, and of the cornco-brachialis muscles. It also shows the insertion of the pectoralis minor, the tendon of which protrudes as a stub at the inner side of the coracoid process in this diagram.
Although it is over twenty years since the above paper was written, I have very little of importance to add or subtract from it. I followed the two cases for many years and the results continued to be satisfactory. Although the second case never had perfect function in his shoulder, he could do all sorts of farm and stable work without complaint. As he worked for a neighbor, I had frequent opportunity to observe him for over ten years.
There is a point in the quoted paragraph which might cause confusion. At that time, 1906, I did not realize that the stooping posture was such a great help in testing mobility in the scapulo-humeral joint. One may get the impression, when examining a patient in the upright position, that scapulo-humeral adhesions exist, and yet in the stooping posture, positive proof will be given that the joint is movable. It is important for the reader to understand at once that scapulo-humeral passive mobility is a sine qua non for the diagnosis of a complete rupture of the supraspinatus, and that in the stooping posture this mobility is much less inhibited by pain and spasm. I did not fully appreciate this point in 1906, and even in 1911 I had hardly grasped it, and did not accent it enough in the above paper. It will be discussed later in this chapter.
The only other point which I desire to correct is in the next to the last paragraph. I do not think I was justified in making such a general statement as "usually these heal satisfactorily if the inflamed portion of the bursa over them is clipped away with scissors," for I am still in doubt as to how to treat the incomplete ruptures.
I have really little more than I had in 1911 to give to the profession in this book, except that repeated experience with the same signs, symptoms, operative findings and follow-up have increased my confidence in the accuracy of my former observations and opinions. During these years I have only operated upon about forty belated cases, although I have made the diagnosis over a hundred times. My results have been good but by no means perfect, because I never see these cases in their early stages, when I am sure the operations would be easy and the results entirely satisfactory. This book aims to try to teach the practicing physicians, who see the cases soon after the injury, how to recognize this lesion immediately, and to rush the patient to a competent surgeon as promptly as if the patient had a broken arm—a much less disabling accident. As in acute appendicitis, early recognition and prompt operation are of the utmost importance. The remainder of this chapter will therefore be devoted to a more detailed discussion of the symptoms.
.jpg)
FIGURE 39. RUPTURE OF THE SUPRASPINATUS
A schematic posterior view of a case of ruptured supraspinatus, to show the posterior short rotators and the sulcus and eminence formed where rupture of the supraspinatus has occurred. The acromion has been sawed off at its base. The reader should study the frontispiece and the next figure in connection with this one.
The size of the rent in the tendon is an important factor since the degree of the severity of each symptom may vary with the extent of the rupture. It seems best to discuss first the symptoms of those cases where the rent is large, as in the two cases which I first reported and which I have called "complete." This means that at least that portion of the conjoined tendinous insertions supplied by the supraspinatus has been torn away, with or without portions of the adjacent tendons. These are the cases which should certainly have the benefit of immediate operation. I do not at present advocate operating upon incomplete cases, for it is likely that after a few months they may heal in whole or in part. On the other hand, there is good reason to believe that the complete ruptures which make an open communication between the joint and the bursa never do heal entirely unless sutured. In other words, the symptoms have had to be pretty pronounced in order to make me willing to operate. It is significant that almost invariably the rent in the tendon has been found to be larger than anticipated. I have perhaps been over-conservative in deciding to operate, but the reader must remember that I have taken the responsibility of doing an operation which is not generally practiced, and naturally I have been somewhat cautious. It is my sincere belief, however, that a small exploratory incision is harmless and that the practice of promptly making such an incision in acute, doubtful cases is to be encouraged, provided the operator has carefully studied the anatomy of the region.
Almost all surgical operations which are now standard procedures had similar histories. Many human sacrifices were required to teach us not to delay when the symptoms strongly suggested appendicitis, perforated duodenal ulcers or intestinal obstruction. The fact that death occurs when we procrastinate in these serious cases has made us, in the public eye, more to blame for delay than for making negative explorations. The surgeon who does explorations on these injured shoulders might be criticized today and yet a few years hence be blamed for the failure to do them. Moreover, the laboring man with a shoulder injury has not yet been educated to dread this particular lesion as he has been to fear appendicitis.
.jpg)
FIGURE 40. X-RAY OF SPECIMEN SHOWN IN FRONTISPIECE Owing to the fact that it had been dissected, air has entered both the joint and the bursa, somewhat after the manner indicated in the cover design. It suggests appearances which we might see if we used air or opaque fluid injections in the bursa and joint. It shows a little irregularity on the surface of the tuberosity, which in the painting gives the appearance that I have called a " volcano "; i.e., a small eminence which has a craterlike place in its center. These little eminences are found in many old cases of ruptured supraspinatus. They may represent a productive osteitis due to irritation from contact with the acromion during elevation. The figure also shows two small caverns such as those illustrated in Plate V, Fig. 1 and Fig. 2. I am not sure just what these caverns indicate.
The account of symptoms given in my 1931 paper before the American College of Surgeons was presented in a twenty-minute talk, and while I still think it accurate, I am not satisfied with its arrangement nor with the amount of detail its time limit permitted. The immediate symptoms were not separated as they should have been from those that supervene later in the course of the disability. The early signs should have been emphasized, because success in treatment must depend largely on prompt diagnosis. It is easy enough to recognize one of these cases when atrophy has developed and the lapse of time has shown the persistent character of the lesion, but to make the diagnosis on the day of, or on the day after, an injury is quite another matter.
Probably insurance records would show that 80 or 90 per cent of employees complaining of shoulder "strains," return to work within three months. Certainly we could not recommend exploratory incision of the bursa in all of these cases in order to detect perhaps 10 or even 20 per cent where the rupture would be complete. When we have learned just what to do when we find minor ruptures or tendinitis, it may become wise to make such incisions as a routine, but at present the bill for negative explorations would be far too large. I contend that it is possible to detect the severe cases.
CERTAIN CONDITIONS, SYMPTOMS AND SIGNS WHICH INDICATE COMPLETE RUPTURE OF THE SUPRASPINATUS TENDON AND WHICH SHOULD BE PRESENT WITHIN TWENTY-FOUR HOURS AFTER THE ACCIDENT.
(1) Occupation—labor.
(2) Age—over 40.
(3) No symptoms in shoulder prior to accident.
(4) Adequate injury—usually a fall.
(5) Immediate sharp, brief pain.
(6) Severe pain on following night.
(7) Loss of power in elevation of the arm.
(8) Negative X-ray.
(9) Little, if any, restriction when stooping.
(10) Faulty scapulo-humeral rhythm.
(11) A tender point,
(12) a sulcus, and
(13) an eminence
(14) at the insertion of the supraspinatus,
(15) which cause a jog,
(16) a wince and
(17) soft crepitus as the tuberosity
(18) disappears under the acromion when the arm is elevated, and usually also, as it reappears during descent of the arm.
Here are eighteen conditions to be fulfilled—an especially exacting syndrome. If such a syndrome is present I do feel that not only is exploration indicated but that it should be strongly urged, for immediate suture should be a simple and successful operation. Delay means retraction of the tendon and a much more serious problem.
I feel confident that this syndrome must exist, although I admit that I have never seen one of these cases within twenty-four hours of an injury. My best way of knowing the immediate symptoms is from the accounts of the patients or of their physicians given weeks or months after the injuries. Moreover, since these same symptoms are found at varying periods from three weeks to many years after the accidents, and do not vary much with the lapse of time, either in quality or in degree, it is likely that they were present at first. In a case in which they were all typical I should be positive of the diagnosis, and should urge operation. If several of the conditions were not fulfilled, it would influence me against operation, but if there were doubt, a negative exploration, if correctly performed, is a trivial matter, although the patient must be hospitalized in case a rupture is found.
If suture is done he should remain in the hospital for about ten days; if the exploration is negative he might well be discharged in twenty-four hours. These eighteen points will be discussed in more detail in numerical order.
(1) Occupation. The great majority of cases must belong to the laboring classes, for I have seen only one case in a person whose occupation did not or had not required heavy work. This suggests that overuse as well as increased liability to accident may be a contributory cause. The occupations are given serially in the following paragraph because if they were tabulated the list would not give the same impression of sequence which is presented by patients as they come for examination. On looking over these occupations the reader should contrast them with those in the following three paragraphs which are the occupations of patients who have had calcified deposits, tendinitis and partial rupture.
COMPLETE RUPTURE OP THE SUPRASPINATUS (100 Cases) Women 8%
Housewife, hostler, plasterer, street cleaner, housewife, coal-heaver, waiter, paper cutter, laborer, housewife, marble worker, currier, cooper, housewife, stationary engineer, two laborers, longshoreman, wrecker, teamster, two laborers, steamfitter, three laborers, truck driver, stock fitter, cook, stableman, painter, two laborers, truck driver, laborer, lineman, lather, farmer, three laborers, harness maker, wood molder, planer, electrician, plumber, mechanic's helper, laborer, roofer, laborer, longshoreman, riveter, two laborers, porter, cooper, two laborers, steamfitter, laborer, lather, steamfitter, laborer, stationary engineer, laborer, store clerk, carpenter, laborer, night watchman, longshoreman, laborer, taxi driver, lineman, laborer, painter, coal-heaver, laborer, foreman, truck driver, laborer, construction, painter, laborer, rubber worker, laborer, painter, laborer, carpenter, meat cutter, floor layer, stitcher, two laborers, housewife, foreman, laborer, store clerk, burnisher, teamster, laborer.
CALCIFIED DEPOSIT (100 Cases) Women 34%
Housewife, two no occupation, two physicians, chemist, physician, superintendent, two physicians, business, no occupation, business, manufacturer, architect, business, three physicians, milk delivery, supervisor, ironworker, housewife, filing clerk, physician, machinist, histologist, housewife, physician, business, no occupation, physician, no occupation, pipefitter, stenographer, no occupation, physician, garage, postman, business, waitress, musician, shipper, laborer, bookkeeper, machine tender, porter, teacher, laborer, housewife, broker, housewife, business, baker's helper, two salesmen, organist, weaver, housewife, shoemaker, forewoman, box-maker, two laborers, housewife, shoe machinist, farmer, housewife, advertising, paper mill, housewife, surgeon, real estate, advertising, housewife, machinist, boxmaker, store manager, wool handler, laborer, physician, truck driver, shoe worker, teacher, knitting mills, housewife, plasterer, laborer, shoe stitcher, clerical, physician, treasurer, investments, laborer, housewife, laborer, beauty parlor, manufacturer, salesman, manufacturer.
TENDINITIS (100 Cases) Women 58%
Two housewives, two no occupation, army officer, two housewives, carpenter, tailor, nurse, no occupation, tailor, nurse, business, P. O. clerk, secretary, three housewives, no occupation, physician, maid, coppersmith, merchant, housewife, jeweler, minister, harnessmaker, housewife, hostler, tailoress, storekeeper, priest, no occupation, photographer, housewife, professor, housewife, carpenter, starter, housewife, shoe laster, housewife, two no occupation, housewife, roofer, civil engineer, two housewives, cigar maker, judge, shoe manufacturer, no occupation, nurse, three housewives, physician, housewife, laborer, two housewives, physician, two housewives, store clerk, housewife, social worker, housewife, insurance broker, factory worker, two housewives, desk work, social worker, salesman, food checker, housewife, consulting engineer, banker, physician, invalid, two housewives, nurse, laundry, writer, surgeon, two housewives, two physicians, foreman, lawyer, grocer, executive secretary, nurse, public accountant, no occupation.
PARTIAL RUPTURE (100 Cases) Women 11%
Three laborers, farmer, carpenter, eight laborers, baker, plumber, laborer, housewife, two laborers, carpenter, housewife, painter, laborer, mechanic, garage, two laborers, writer, three laborers, physician, laborer, carpenter, teamster, laborer, carpenter, laborer, machinist, laborer, housewife, teamster, cook, stone mason, bricklayer, carpenter, three laborers, store, housewife, laborer, mechanic, housewife, store clerk, cook, machine oiler, laborer, two housewives, insurance, store, business, janitor, hoisting engineer, painter, meat cutter, three laborers, florist, two laborers, ironworker, nurse, gardener, shoe factory, clerk, plasterer, lawyer, laborer, no occupation, student, bartender, manager, housewife, laborer, foreman, bricklayer, horseman, two laborers, nurse, farmer, machinist, real estate, gardener, laborer, housewife, tailor.
Both occupation and sex are of importance in the diagnosis of shoulder conditions. Men who have done heavy labor are typical subjects for complete ruptures of the supraspinatus, and women of the so-called "leisure class," for tendinitis (frozen shoulder). Calcified deposits are more characteristic of the class who have gainful but not laborious occupations (the white collar class) ; i.e., they are not usually found in inactive people. Partial ruptures are also in the main characteristic of men of the laboring group, but they may occur in the more active and athletic members of the leisured class, both in men and in women.
These observations were already made from general impressions in the course of my practice, but they are in part confirmed by the above analysis of the occupations of 400 cases. The detailed accounts which each patient has given of his or her occupation and other activities, are of even greater weight in confirming my own impressions. For instance, the term housewife may apply to a woman who does all the work and washing for a large family, or to a lady who scarcely uses her arms, or to an active wife who plays golf, sends out her washing and only occasionally uses her kitchenette. The percentage of women varies greatly in the different classes, eight per cent, eleven per cent, fifty-eight per cent and thirty-four per cent. The eight cases of complete rupture and eleven of the fifteen cases of partial rupture were women whose work was really laborious. The fifty-eight tendinitis cases were chiefly women of the leisure class and the thirty-four calcified cases were active single women or wives.
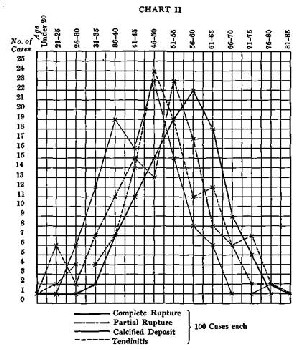
(2) Age. The four clinical entities also affect different age groups. Young persons below twenty-five seldom have any of these conditions. Apparently in young people the tendon is stronger than the bone in which it is inserted, and stresses, which in later life would break the tendon, cause fracture of the bone or separation of the tuberosity. Chart I shows that the four entities affect, in the main, persons in the latter half of life, and that the occurrence of tendinitis both of the calcified and uncalcified forms precedes the peaks of incidence of the ruptures, partial and complete, by about five to ten years. The curves of the two forms of tendinitis, calcified and uncalcified, have their peaks at the same period, but the rise of the curve is distinctly earlier in the calcified form. These facts suggest that injuries of the tendon prior to the thirtieth year either are rare or that the tendons are capable of normal repair. Then follows a period when repair is uncertain and is apt to be complicated by the deposit of calcium. Later even this incomplete repair fails.
WOMEN—CHART III
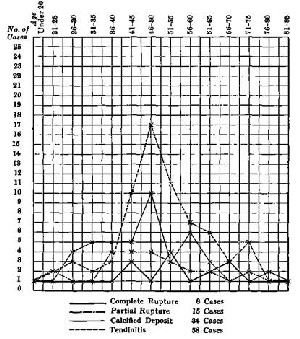
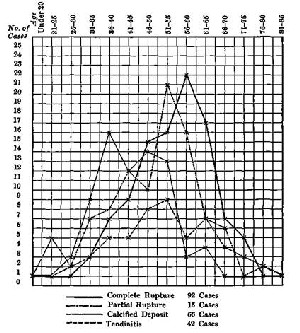
If we chart separately the male and female cases there is a marked contrast. The curve of the female cases suggests that tendinitis, both calcified and uncalcified, may be related to the menopause or to the age when the teeth begin to loosen. By comparison of the two charts we find that calcified deposits apparently occur somewhat earlier in males than in females, and their occurrence tends to diminish at the period when they are highest in the female. The contrast of Chart II and Chart III makes it very clear that the more serious forms of rupture of the supraspinatus are characteristic of the male toward the end of his laboring days. The period of life shown in all the curves is that in which the teeth are usually in decay. If these charts are made without separating the cases in four entities the contrast between the ages of males and females is even greater, so that the coincidence with the menopause is more striking.
MEN—CHART IV
(3) The history of a previously painless and useful arm is unreliable for two main reasons. First,—previous troubles may have been forgotten. Men of the laboring classes put up with a great deal of soreness and pain and forget it easily. Such a matter as an attack of bursitis years before, may readily be forgotten. I would rather
have the history of previous troubles from a man's wife than from the man himself. I am inclined to think that in many cases where complete rupture has occurred, there may have been previous minor troubles, which might have indicated either partial rupture of a few fibers, or a "calcined deposit." However, my records do not show this, for in only nine of a hundred cases could a history of previous trouble be obtained.
The second reason is that men may lie as well as forget. The statements of employer and fellow workmen are sometimes more accurate than the patient's own. Patients may conceal previous trouble to avoid losing compensation.
The other shoulder should always be examined in these cases, for occasionally one finds signs of a partially ruptured tendon or of chronic bursitis there, although no complaint is made of symptoms. This would, of course, be very suggestive of preexisting disease in the injured shoulder. However, we must not forget that a rupture may occur as a bona fide injury in degenerated or diseased tendon.
(4) Adequate injury seems pretty well illustrated by the following brief accounts of the accidents in twenty-one successive cases which were proved by operation, and in seventy-nine others in which the diagnosis was made but not proved.
ACCIDENTS (Operated Supraspinatus Cases)
57. "Fell taking down an old gallery."
75. "On this date (Aug. 25, 1922) he was engaged with others in hoisting lumber, when a plank slipped off the hoist and struck him in the side knocking him down."
83. "On Jan. 17th, 1923, he fell downstairs and injured his left shoulder."
88. "On Feb. 1st, 1926, while at work he was pulling a heavy case along the floor with a hook. The hook slipped and as he caught his balance he felt something snap in his shoulder accompanied and followed by intense pain."
89. " When getting off truck caught his hand in fly wheel. Cuts of hand."
96. "On April 4th, 1927, he slipped on a concrete floor and injured his left shoulder."
97. "On Nov. 8th, 1926, he was pushing a freight car with another man, using bars. His bar slipped and he fell down wrenching his left shoulder."
98. "Six weeks ago he had slipped on the ice while at work and had injured his right shoulder. He fell on his back striking his elbow, but had no bruise on the elbow. (It is probable he threw up his arm to get his balance.)"
102. "On Nov. 2nd, 1927, he was piling some 100-lb. sacks of beans with another man who stood above him and received the sacks as he threw them up. On one throw the other man failed to connect with the sack and the entire weight came on the patient's right arm. He felt something in his shoulder snap with a sharp pain."
106. "On January 20th, 1928, he was cranking his truck, which he uses to deliver cans of ice cream. The engine backfired and he felt a sharp pain in his right shoulder."
107. "On Jan. 18th, 1928, she fell on the floor of the kitchen where she works and dislocated her left shoulder."
108. "At some time in July (date uncertain) while at work he was turning a board and felt something snap in his right upper arm about the middle, in the region of the long head of the biceps. There was a sharp pain which went away in a few minutes."
112. "On March 10, 1928, he was wheeling a barrow up into a barn when he slipped and fell forward on the barrow, but did not let go of the handles."
115. "On August 21st, 1928, about 1.30 P.M., slipped and fell from piazza roof, striking the edge of the piazza floor with his right arm in abduction. Had immediate pain in shoulder and arm."
119. "Day before Thanksgiving, Nov., 1928, fell off staging three feet high. Walked backwards off."
123. "On Jan. 14th, 1929, he slipped on an icy platform and hit on his left elbow."
127. "On Oct. 17, 1929, was handling 2x4 lumber and stepped in a hole. Fell against left shoulder on pile of lumber, hitting on elbow."
128. "He slipped on the ice near a building and fell, striking the side of his right shoulder against a low step. This is what he says, but such a fall as that would probably be impossible. It is more likely that he threw his arm up as he fell."
129. "On October 24th, while piling some pipe, he was standing on a pile of pipe which rolled under his feet and he fell between two piles of pipes."
185. "He slipped on the ice and fell. After he got up, he found that he could not raise the left arm."
137. "On May 13, 1930, he had a fracture near the left elbow which healed satisfactorily and he went back to work about September 1st. On October 7th, in Andover, he fell and dislocated his left shoulder."
ACCIDENTS (Unoperated Supraspinatus Cases)
". . . he was doing some overhead work standing on a support twelve or fifteen inches high. The support slipped and he fell on his right hand and elbow, and then forward on his shoulder." ". . . he was pulling on a rope which suddenly gave way. He fell to the ground with his right arm below and behind him. He felt a sharp pain in the shoulder as if a bone had broken." ". . . he fell about ten feet while at work and injured his shoulder." ". . . he had been hit by an automobile, knocked down and taken to the Boston City Hospital. His shoulder had been injured." ". . . he was cranking his truck, and had a kick back. He thinks the handle struck him on the lower part of his upper right arm, but his shoulder was w.renched." "... when walking in a dark passageway, he stepped over some steps and in trying to save himself caught with his left arm on the wall, but kept his feet. He had a violent pain in his left shoulder but pulled himself together and went to his next job." ". .. he was struck on the left shoulder by a falling bale of hemp while at work. He was knocked down and much shaken up, but pulled himself together and continued to work the rest of the afternoon with his right hand." "Fell off wagon when unloading barrels. Hurt badly at time and went to Camb. Relief Hosp." ". . . he was lifting a barrel and something snapped in his shoulder, since which he has been unable to work." ". . . he tripped on a rolling log and fell injuring his left shoulder." ". . . he fell down some stairs and injured his right shoulder." ". . . the employee slipped on a loose plank and injured his left shoulder and right foot." ". . . he was pulling on a chain fall and something slipped in the right shoulder." ". . . he was jammed between a moving truck and the side of a building. Fortunately, he was near the corner of the building and the moving truck carried him around the corner, squeezing him from side to side as it did so. His left arm immediately became powerless." ". . . he fell from a staging and injured his right shoulder and has not yet recovered the use of it for anything requiring the function of abduction." ". . . he was filling a wagon with coal when the horses started and he fell in between the wagon and the side of the coal-pocket." ". . . he fell forward at the top of a flight of stairs and injured his shoulder as he supposed by hitting some beams." "A frame which he was moving dropped and to prevent it striking his feet stepped aside, losing his balance and falling to the floor." ". . . she felt something snap in her shoulder (left) when raising some wet clothes on a pole to put them in a laundry machine." ". . . while raking grass on a steep bank, he slipped and injured his left shoulder." ". . . as he was stepping out of a tip cart on the hub of the wheel, he slipped and fell heavily to the ground injuring his left shoulder and also his right shoulder to some extent." ". . . the employee was carrying a plank with another man, when one of the planks on which he was walking gave way, letting part of his body through the pier so that he sustained injuries to his left shoulder, arm and leg." ". . . she fell over a bag of soles and injured her right shoulder." ". . . he slipped off a plank and fell headlong to the floor, about four feet." ". . . large heavy car six or eight feet on the side. On this occasion the car skipped the track in spite of his efforts to prevent it, striking him on the left arm." ". . . he says that he was using his truck to load heavy rubber bales weighing about 350 lbs. each. He had put the edge of his truck under one such bale and reached forward with his right hand to pull the bale toward him on to the truck. As he pulled, he felt something give in his right shoulder." ". . . he was helping with other men, to pull a heavy truck, when he felt something give way in his right shoulder." "He was carrying a roll of leather and fell on the floor in the room where he usually worked." ". . . he fell from his truck and injured his left shoulder." ". . . he fell thirty feet from a staging and was badly bruised all over." ". . . he was on a lumber pile helping to load a truck. He was using a pick to drag the lumber. The pick slipped and he felt a sudden pain and something snapped in his arm at the right shoulder. His arm fell limp at his side." ". . . he slipped on some stairs and injured his left shoulder. . . ." ". . . fell among some barrels in the hold of a vessel and struck his right shoulder again." Had had previous similar accident six years ago, and never full use of arm since. ". . . while working in a meat market in Nantucket, he slipped on going out of the ice chest and injured his right shoulder." ". . . while carrying rubbish on an incline in the factory where he works, he fell and injured his right shoulder. As he says, 'it went dead immediately.'" "He was piling wool at the time, lost his balance and fell from one bale to some other bales not far below. As he fell he felt something snap in his shoulder which did not hurt him very badly at the time. . . ." ". . . slipped on ice in street." ". . . while working on a flat-car he fell and struck his right shoulder on the side of the car." "While at work in the factory in Lawrence ... he was in an elevator holding a heavy plank in both hands to steady it. One end of the plank was on the floor of the elevator and it stood vertically. Some one below started the elevator downward and then upward. As it went up it thrust the top of the plank violently against the top of the well. This shattered the heavy plank just above his hands with extreme violence and he was thrown into the corner of the car in a heap." ". . . he fell off the back of a load of straw and injured his shoulder." ". . . he again fell downstairs—only a few steps—and again injured his right shoulder." " Slipped and fell, and a box or case fell over on him." ". . . while directing some work where a floor was being replaced and the boards were up, he tripped on a beam and fell on his right side against another beam, probably breaking some ribs." ". . . he received an injury to his left shoulder when trying to move a large rock with a pitchfork. He felt something snap in his shoulder joint and suffered a sharp, severe pain at the same time." "He injured his right shoulder by falling from a truck." ". . . he was pulling some lumber off a truck and when it slid off quicker than he expected he fell backward and injured his left shoulder." ". . . he fell four feet, striking on the pavement, and inj ured his left shoulder." "... he slipped on an oily floor, and hurt his right shoulder and left shin." ". . . he fell from a staging about six feet to the floor below, and injured his right shoulder." ". . . he fell from a ladder and sustained injuries to the left shoulder and ribs." ". . . he was on a roof sawing a plank, and was standing on an extension ladder, which fell with him thirty-one feet to the ground. His right shoulder was injured, and his nose was cut" "Strap from machine fell off wheel and hit patient on right shoulder." ". . . he was working with others on a bridge in Rumford, Maine, helping to receive some cement in a frame from a bucket. In some manner, the bucket swung in the wrong direction and the patient fell from the bridge a distance of fifty feet." ". . . he was lifting a concrete block and felt something give in his left shoulder." ". . . he fell injuring his left shoulder." ". . . he had started to crank a hoisting truck when the starter began to work and the crank flew round and struck him on the right shoulder." "Slipped on ice." "Fell yesterday and sustained a contusion over outer end of right clavicle." ". . . while helping to unload a truck, a derrick knocked down a platform above him, and something, probably a heavy plank, fell on him and others working with him. He was knocked out by the blow, and cannot describe exactly the manner in which the plank struck him, but he knows it injured his shoulder and elbow and there was blood streaming down his arm." "He was pulling hard on a gunny sack, which gave way, and he fell over and thinks he struck his right shoulder." ". . . she tripped and fell on the floor at her work. She dislocated her right shoulder, bruised her knees severely and cut her face." "He was standing on stony ground swinging a sledge hammer, when he had to step back quickly. As he did so, he lost his footing and the sledge hammer, which he was swinging, carried on around his body so that his left shoulder was in an awkward position. He felt something snap in the left shoulder."
One may interpret the mechanism which produces this injury in several ways, but a sudden character is common to all of the accidents, which are generally falls. It is my belief that the rupture usually takes place from sudden elevation of the arm in attempting to regain balance, particularly if the hand is at the same time grasping a heavy object. Under these conditions a tremendous strain must be suddenly thrown on this little tendon as it attempts to quickly overcome the inertia of the arm, and perhaps, in addition, that of some heavy object held in the hand. In my first case, the woman attempted to throw a heavy, wet blanket over a clothes-line. It seems to me that this case, like a "slowed down movie," typifies the kind of strain which occurred in most of the other accidents. I believe that the even more sudden effort to regain balance during a fall caused the damage, probably before the patients struck the ground. For anatomic reasons one cannot, in falling, strike on the supraspinatus, because it is protected by the acromion.
Undoubtedly, however, in some cases, the tendon may have been torn in conjunction with dislocations, because of the leverage of the humerus on the fulcrum of the acromion. This mechanism will be explained in Chapter IX.
(5) A sharp pain in the shoulder at the time of the accident is almost always spoken of, although occasionally complaint of it is not volunteered. Sometimes patients say that they have felt something actually snap and think that they have broken a bone. Sometimes they feel that something has struck them on the shoulder. It has been explained on page 9 in the chapter on anatomy that histories of striking on the head of the humerus are unreliable because the acromion intervenes, and on page 144 that in falling, the arm is usually raised before the top of the shoulder can strike the ground. Consequently it seems to me that these tendons must usually be ruptured by indirect violence or sudden efforts of the muscles to overcome the inertia of the dependent arm, especially if there is a weight as a pick or shovel in the hand at the time, or the hand grasps something to save the man a fall. Often the fall is so sudden and the man so confused that the only thing he can understand is that he has hurt his shoulder and attributes the pain to having hit something as he fell.
(6) So far as I can judge from histories, there is then usually an interim of a few hours after the acute, immediate pain has somewhat subsided before the more severe pain comes on. Often the employee does not even consult a doctor at once, but tries to work the day out, favoring his arm. Perhaps he does not report the accident to his foreman. In the evening the pain becomes worse, and later in the night intolerable. He calls the doctor, or sits up in a chair, or "walks the floor." Next day he is pretty sure to report that he cannot work, but may persuade an accommodating foreman to let him "hang around" for a day or two until he gets better. These patients usually think the injury of no great consequence and expect "to have it wear off." This hopefulness is generally confirmed by the doctor's opinion, who perhaps may never have heard that such lesions occur. This attitude of mind of both patient and doctor is the main cause of delay in diagnosis and appropriate treatment.
It seems to me that the following theory is the probable explanation of the interim between the sharp pain when rupture occurs and the intense pain which appears some hours later. These tendons are not very vascular, and when they tear, there is probably very little bleeding; what there is, would come from the tissue between the bursa and the tendon. The interim spoken of would come during the period it would take this slight hemorrhage to distend the joint and bursa somewhat, i.e., enough to start a tension pain. This would create some spasm, and the tension caused by this would stop the slight bleeding. It would take several nights or perhaps a week for tension and spasm to subside and the hemorrhage to absorb. During this period the acute pain would continue.
(7) Inability to raise the arm is a constant symptom, but one must be on guard not to mistake unwillingness for inability. After almost any shoulder injury there may be pain when attempt is made to raise the arm, owing to the fact that the head of the humerus has to be forced upward to gain its fulcrum on the glenoid. The mere fact that the muscles have to exert tension to do this, causes pain in whatever structure about the shoulder may be injured. Therefore, the examiner must be sure that an honest effort is made to ignore the pain and elevate the humerus. It takes experience to tell whether such an effort is made, and one judges it by the degree of tension palpable in the deltoid. Even in the case of trivial injuries, such as ruptures of a few fibers of the supra- or infraspinatus, the symptom of inability to raise the arm may be pronounced, simply from the fact that the power to exert the appropriate muscles is inhibited by sensitiveness to pain. As explained on page 59, the deltoid needs the assistance of the supraspinatus and of the short rotators to hold the head of the bone on its fulcrum in order to have proper direction for its power; If the supraspinatus is torn, contraction of the deltoid brings the arm upward on the vertical axis of the humerus, and the amount the shoulder is raised will depend on the amount that the scapula, moving via the. sterno-clavicular joint and at the acromio-clavicular joint, can rise and rotate on the chest wall.
Formerly I thought that it was necessary to have this symptom of inability to raise the arm absolutely demonstrable in order to make the diagnosis of rupture of the supraspinatus, but experience has shown that, even when the supraspinatus is torn across its full width, the other short rotators can sometimes hold the head of the humerus on its fulcrum sufficiently to permit the patient to weakly perform elevation. However, as will be explained under No. 10, this elevation is never accomplished with a normal scapulo-humeral rhythm.
(8) A negative X-ray is almost always reported after these in juries. I believe that in the near future we shall be able to make the X-ray of more use in this diagnosis, either by using injections into the joint of non-radiable fluid, or by developing a soft tissue technique which will show the rupture. However, at present, negative X-rays are the rule, for ruptures which do not involve the bony facet of insertion are not shown in the film. A negative X-ray is of some positive importance, however, for it rules out the two conditions which are likely to make confusion in the diagnosis, that is, fracture of the
greater tuberosity and the presence of calcified material in the tendon. In long-standing cases changes in the structure of the trabec-ulae of the tuberosity which may be shown by the X-ray do take place. These are described on page 92.
(9) In the symptom complex of this condition, lack of restriction of motion takes a very important part, and this lack of restriction can be best determined when the patient is stooping from the hips with the knees extended. The patient should stoop (Fig. 47) to the horizontal position, letting the arms hang loosely toward the floor. In this position the deltoid is relaxed and there is no fulcrum needed in order to have the arm passively raised, i.e.-, brought forward into complete elevation (quadruped extension) ; in fact, even if this is not passively done, the patient has to exert but little muscular power
to swing the arm forward into this position. This he is usually able to do without much pain. The examiner may then hold one hand on the scapula and with the other raise the lower end of the humerus, so that he takes the full weight of the arm and permits the patient to stand upright with the arm still in complete elevation. Such a procedure eifectually rules out restriction from adhesions. Even if the supraspinatus is torn, the patient can retain the arm in this up right position. If he stoops again he can lower it without much pain, and then if he rises to the upright position with the arm relaxed,
the humerus will, by gravity alone, come into its normal position at the side of the body.
When I say that lack of restriction is an essential symptom, I must not be taken too literally, for there is often, in fact usually, in these cases, a very little restriction in extreme elevation and in rotation, probably due to the presence of fluid.
(10) Faulty scapulo-humeral rhythm is a sine qua non for this diagnosis. When one sees a patient who in raising the arm lets it ascend to the horizontal while maintaining (quadruped) flexion of the scapulo-humeral joint, and then slowly and painfully (perhaps with a little help) proceeds to complete elevation by motion in the scapulo-humeral joint, and finds that when the patient 'allows the arm to descend, he keeps the scapula and humerus fixed in (quadruped) extension until he reaches the horizontal, and then quickly flexes it, a presumptive diagnosis oi rupture of the supraspinatus
can be made. Ascent in flexion, descent in extension, might be a slogan for students to learn in this connection. To express this lack of scapulo-humeral rhythm in other words, we may say that the normal ratios of the movements of the joints in elevating the arm, explained on page 59, disappear. Instead, in the first part of the movement only the motions of the scapula on the chest wall are concerned; then the relations of the humerus and scapula change, wholly above the horizontal. In the descent of the arm the reverse is the case—no scapulohumeral motion takes place above the horizontal, but all below it. While the symptom is a sine qua non to the diagnosis of complete rupture of the supraspinatus, it is also present in most cases of minor ruptures and in many cases of calcified deposits. It therefore is an indispensable but not a pathognomonic sign.
(11) The tender or sensitive point is not complained of by the patient as a rule, and in fact he is unconscious of its exact location until the examiner finds it, when he usually says: "You have your finger right on it." Without your aid in locating it he will perhaps know that there is a tender point, but locate it deep under the acromion or even in the spasmodic deltoid muscle down near its point of insertion. In fact, the lower portion of the deltoid is usually also tender. Examination of this part of this muscle in all these patients nearly always shows that there is some thickening and sensitiveness, as compared to the normal side. In the old, chronic cases the sensitiveness at the point of rupture may not be very noticeable, and even when the exact point is pressed the patient will hardly admit that it is tender. Presumably in fresh cases it would be especially sensitive.
.jpg)
FIGURE 41. POSITION OF HANDS FOR EXAMINATION OF SHOULDER
The left thumb lies along the depression below the spine of the scapula and the tip of the forefinger is just anterior to the acromion. The other three fingers cross and hold the clavicle. Thus the shoulder girdle is firmly held and any motion of the scapulo-humeral joint is at once detected.
In speaking of the 11th, one is necessarily obliged to consider the remaining symptoms, since the tender point is at the gap between the ends of the torn tendon, and this gap is the reason for the sulcus and eminence, which may be felt just anterior to the edge of the acromion, when the arm is in dorsal flexion. If the examiner remembers his anatomy, the tender point, sulcus and eminence will be found to be at or near the insertion of the tendon of the supraspinatus. It is the passing of this irregular sulcus and eminence under the acromion and acromio-clavicular ligament which causes a jog, a wince, and a soft crepitus, as the sensitive, irregular base of the bursa disappears under the acromion when the arm is brought forward by the examiner. The two figures (41 and 42) present the condition, it seems to me, more vividly than could any description. However, I will give a few brief additional points under each one of the remaining headings.
.jpg)
FIGURE 42. TIP OF FINGER PRESSING ON EMINENCE AND ON SULCUS
The plane of this diagram is halfway between the coronal and sagittal.It is, perhaps, the most important diagram in the book for the reader entirely to understand, for it is the ability to put the finger in this position which enables one to make the clinical diagnosis of rupture of the supraspinatus tendon. The dotted line represents the contour of the bursa. Compare this with Figure 44, which shows the contour of the bursa when filled with the calcified material, and also with Plate II, Fig.3, which shows a large calcified deposit in exactly the situation in which the rupture lies in this diagram. In this one the sulcus is immediately under the tip of the finger and the' eminence just external to it, but in Figure 3 the eminence would be just under the finger. Therefore, as explained on page 148, the tender point in a case of rupture is represented by a depression, but in cases of calcified deposit, by an eminence at the corresponding position.
(12) The sulcus is just about big enough to be filled by the tip of the finger, as indicated in the diagram. It is nearly always found to be larger at operation than one would guess from palpation before incision.
(13) The eminence is an eminence only by contrast with the sulcus. It consists of normal tuberosity with perhaps a remnant of the tendon attached to it. In elderly men without injury to the shoulder one can often feel the tuberosity because the tendon is more or less atrophied, so that at times it is hard to be sure whether the tendon is torn or merely atrophic. However, in most cases of ruptured supraspinatus the eminence is conspicuously large and one is quite sure of its existence. It is well to say here that the eminence which is found in cases of calcified deposit is not on the tuberosity itself, but proximal to the tuberosity in the tendon at just the point where ruptures so often occur. Furthermore, the tenderness is usually greater on the eminence in cases of calcified deposit than it is on the eminence in the cases we are speaking of.
(14) As may be seen under Pathology, the supraspinatus is nearly always torn if any of the other short rotators are, but it is very common to have portions of the adjacent tendons torn, so that the tenderness, eminence and sulcus may be a little internal or external to the mid-point of the insertion of the supraspinatus itself. This latter may be determined pretty accurately by placing the forearm in flexion and drawing a line from the mid-point of the flexure of the elbow to the mid-point of the head of the humerus. The bicipital groove lies about its own width external to this line, and the supraspinatus is on the top of this line and to the outer side of it for about three-quarters of an inch. The insertion of the infraspinatus is just external and also partly in front of that of the supraspinatus, for, as explained in Fig. 6, the two insertions nearly cross each other. The insertion of the teres will be found nearly exactly on the mid-point of the head of the humerus on its outer aspect. Be careful, in determining this, that the forearm is flexed at. the elbow and held straight forward. The insertion of the subscapu-laris can be determined by putting the arm in the anatomic position and placing the examiner's forefinger just external to the tip of the coracoid process, which is always palpable, as shown in Fig. 6.
(15) The jog is noticeable to the patient himself, and sometimes is visible as well as palpable to the examiner.
(16) The patient nearly always winces as the jog occurs, but in long-standing cases he may not do so.
(17) The soft crepitus is not like the crepitus in fractures. It is of a more velvety, gristly character. When one has become familiar with it, it is easily distinguished from the kind of crepitus often found in the shoulders of old working men, which resembles the crepitus one frequently feels over the prepatclla and olecranon bursas and about the other joints.
(18) When the sulcus, eminence and tender point have once passed beneath the acromion as the arm is elevated, there is a sense of relief on the part of the patient which is usually apparent in his countenance. When the arm is almost fully elevated (there is often so much fluid in the joint and bursa that absolutely complete elevation is not attained), the patient is relatively comfortable. His pain will appear again when flexion occurs at the level of the shoulder, after the arm has descended with humerus and scapula locked, to a horizontal position. At this time the jog and crepitus are usually again palpable. As this occurs the patient leans toward the affected side and lowers the whole arm quite suddenly.
These eighteen symptoms must be present soon after the accident, but the difficulty is to estimate the degree of the rupture at this time. Partial ruptures must give much the same symptoms as complete ones at this stage, and the degree of spasm must vary, as well as the courage of the patient as he makes a voluntary effort to raise the arm. Immediate diagnosis cannot be easy at this stage. However, the progress of the case makes the diagnosis easier and easier, although valuable time elapses. If exploration is not done these symptoms remain the same and the following points in the course of the case will tend to confirm the diagnosis.
Character of Pain. Practically every patient whom I have seen has given the history that during the first few nights after the accident the pain was severe or intense. Gradually this severe pain changes to a nagging, annoying one, sufficient to greatly interfere with the night's rest, but bearable without drugs. It is usually located near the deltoid insertion far below the actual lesion. Pain of this character continues week after week and with but little change for many months. It is aggravated by the attempt to work, and the patient's resistance to it is gradually lowered as he becomes more and more worn out by restless, painful nights. I am convinced that this pain is very severe as well as prolonged, for I have heard many strong laboring men state that they have never suffered such pain in their lives. It is more the persistence of it than the pain at any one time which wears them out. They often say: "If I could only get a good night's rest I could work during the day." Practically they find that working during the day gives them bad nights, and therefore nearly all of them, in spite of their courage, give up work after a time. Of the series of a hundred cases, only eighteen stated that they had worked for even a brief period. They say that they may go to sleep for a while, but wake with pain in the shoulder or in the region of the insertion of the deltoid, and that they have great difficulty in getting the arm into a comfortable position again. When they do, they go to sleep only to wake up in a few hours for another change of position. Sometimes they get up and walk about or apply hot water bags or other household remedies. It is very characteristic of these cases to have complaint of pain out of proportion to the physical signs, and therefore they receive little sympathy.
Atrophy of the spinati, as shown by prominence of the spine of the scapula, always occurs after these injuries, but does not appear for about three weeks. After it has once appeared it persists, and is apparent for a long time even in the operated cases.
In very few of the cases that I have seen years after the injury was it absent. The atrophy may be more conspicuous in the infraspinatus, which is the larger muscle. Whether the fact that the infraspinatus is always also atrophied, is due to the crossing of its fibers of insertion with those of the supraspinatus so that they are always also torn to some degree, or is due to the fact that the two muscles are supplied by the same nerve, i.e., the suprascapular, I do not know, but it is a fact that atrophy of both is a constant sign. Of course atrophy of these muscles occurs in any chronic condition of real severity affecting a shoulder joint, so that the presence of atrophy does not necessarily indicate this diagnosis, but its absence would he strong evidence against it. In a few long-standing cases I have seen only a small amount of atrophy. It is usually very pronounced. As a rule the deltoid is not much atrophied and may even be hypertrophied.
The general condition of the patient is a factor in diagnosis, for he gets into a vicious circle. He is out of work so that all the muscles of his body become enfeebled. He often cannot afford good food, and he may, therefore, be ill-nourished. Add to this the constant depletion of his energy from restless, painful nights, and we may readily account for the fact that while previously he was a strong, healthy man, he now appears haggard and unhappy.
The mental condition also is poor, for worry on account of inability to work, and that he may never be able to work again, is enhanced by the fact that the physician he consults is unable to tell him the cause of his trouble, and all attempts to relieve him by ordinary remedies absolutely fail. Seeing these cases months after their accident, I am frequently told, "Nothing they have done has done it any good."
The actual physical deterioration from worry is still further aggravated by the doubt that is thrown on their veracity by the physicians employed by the insurer. Usually by the time they are sent to see me some months later, their attitude of mind is defensive, and they at once begin to express their disgust with being told that they ought to go to work and think less about the pain.
This attitude of mind becomes still worse when they are actually accused of hysteria or malingering. They say they want to work. "Do you think I would lie around like this if I could earn $24.00 a week?" They become embittered at their treatment by society in general in spite of the fact that they may still be receiving their compensation.
At length they may lose their self-respect, and brooding over their hard luck take to drink. My second patient was such a case. He had had a good job which he enjoyed; after his injury became discouraged, and evidently decided to let things go and to use up what money he had saved, in drinking as much as he had a mind to. The person for whom he formerly worked, instead of losing sight of him, looked him up, and, realizing that he must have some real trouble with the shoulder, sent him to a doctor who referred him to me. The result of the repair of his tendon was not only that he was able to work, but that he refrained from drinking and worked for ten or more years for the same people who formerly employed him.
Unfortunately the attitude of the relatives of such an old man with a disabled shoulder is apt to become somewhat like that of the doctors who have been unable to diagnose and relieve him. His own family after a while get to think of him as a burden, and since they can see nothing the matter, such as a limp or a deformity, are inclined also to think that he has "laid down" before his time. In recent years, however, we see more signs of sympathy, for the compensation such patients may receive will perhaps be the chief support of the family.
Undoubtedly many such cases eventually turn up as recipients of charity and eventually die in state institutions. It is not surprising to me that the material reported in this book, which was accumulated by Dr. Akerson at a hospital for the indigent, shows such a high percentage of instances of these lesions.
I would venture to predict that if one should see the patients who are chronic nuisances to industrial insurance boards, and the physicians connected with the administration of compensation for industrial injuries, most of those complaining of shoulder disability would have this particular lesion.
Some patients may continue to work. There are rare individuals who, in spite of the disability, have the courage and otherwise sound health to continue to work in spite of the soreness, awkwardness, loss of power, and painful and restless nights. About one-fifth of my series attempted to work for a time before they gave in and sought compensation. I have no doubt that there are others who have never given in.
This is a lesion which tries a man's character, and, since it usually occurs in later life, is often the cause of permanent incapacity, for even if the use of the arm returns in good measure at the end of a year, the patient's habit of work has been destroyed, his muscles have become soft. If he has the courage to go to work again, he will find it difficult to get a job. Those courageous men who do work in spite of the lesion, become more or less free of serious symptoms in from two to five years. As has been explained under Pathology, compensatory changes take place so that the eminence absorbs, the sulcus partially fills, and an excess of fluid allays friction. After several years even the night discomfort disappears, and weakness in abduction, atrophy of the spinati, friction rubs, the fluid sign and occasional pain in certain positions may be the only aftermaths of the injury.
Hypertrophy of the Deltoid. Perhaps it would be better to make this heading "well-developed deltoid as contrasted to the spinati," for the hypertrophy is not striking except when compared to the condition of the spinati. It is a fact that, in the long-standing cases, the deltoid itself is as well developed, or even more so, than that of the other side. I explain this because it has to do most of the abducting work of the arm unaided by the supraspinatus. It not only misses its help, but acts at a disadvantage as explained in Fig. 3. Hence it retains its development or even hypertrophies. My third case had a deltoid like a ham, but at the end of five years he could only feebly perform abduction and could not raise even a slight weight in that hand above his head. He had refused operation.
The Fluid Sign. Among the auxiliary signs and symptoms I find some help from what I call "the fluid sign." I had studied shoulders for many years before I realized how fluid in the true shoulder joint behaves. When the arm is by the side, the fluid sags in the relaxed axillary portion of the capsule. When the arm is elevated the axillary portion of the capsule is stretched tightly below the rounded head of the bone, and the fluid is driven upward where the capsule is now relaxed. In case there is a rupture of the supra-spinatus tendon, the fluid is forced through the gap and distends the bursa in the subdeltoid portion beneath the upper fibers of the deltoid.
Stand behind one of these patients, who is holding both arms as straight as he can toward the ceiling, and you will see that the contours of the two shoulders are quite different. When there is a considerable amount of synovial secretion, absolute complete elevation of the arm is prevented by the mass of fluid. Another interesting point is that when there is fluid the friction is largely prevented as the arm is elevated. When it subsides pain reappears. This phantom improvement by the formation of fluid is not uncommon.
Patients who continue to work in spite of their pain develop fluid, as do people with various affections of the knee. The fluid continually pumping in and out of the bursa dilates it and a true hydrops may result (p. 478). One finds in long-standing cases that the bursa is very large. (See case Fig. 44.) Some fluid, from a dram to an ounce, is a constant operative finding in these cases. It may not be noticed when the bursa is first opened, but if one elevates the arm and puts the axillary portion of the capsule on the stretch, the thick, straw-colored fluid runs out of the wound. Sometimes there is enough to distend the bursa even in the anatomic position, and when the first incision into the bursa is made, it obscures the field and has to be sponged out.
This behavior of the fluid was forced on my attention when I used to put the arm in abduction after suture. This caused the weeping wounds described on p. 248, and this serious and annoying complication led me to reason out the facts.
INCOMPLETE RUPTURE
Although there is no sharp anatomic distinction between complete and incomplete rupture, there is the practical one that cases of the former will not recover completely unless the tendon is sutured, while cases of the latter may heal in a natural manner. One which is typically complete involves the whole supraspinatus tendon, with perhaps parts of the adj acent tendons. One which is typical of the incomplete form need neither involve the whole width nor run through the whole thickness of the tendon. In its minimum phase it may be only an evulsion of a few fibers from the tuberosity; in its maximum phase it would be a borderline case of complete rupture. In its acute phase it may be definitely due to trauma; in its chronic phase the tendinitis overshadows the traumatic history.
The reader who has the patience to finish this book will inevitably remain confused about the lines of distinction which I have attempted to draw among the six most common clinical entities which affect the shoulder, i.e., complete and incomplete tendon ruptures, rim rents, calcified deposits, tendinitis and arthritis. In fact, I must leave the reader puzzled, for I am still puzzled myself. I can only confront him with the puzzle—show him that there is a puzzle. Personally, I believe that these rim rents and incomplete ruptures are the cause of the great majority of sore shoulders, and yet I believe they usually occur in degenerated tendons. For example, a man might have degenerative changes in both shoulders without symptoms and then, after trauma to one tendon, have severe local symptoms without any signs of trouble in the other shoulder.
One cannot even divide complete and incomplete lesions by the criterion of whether or not there is a direct communication from the bursa to the joint through the rupture, for the size of the opening is important also. Yet splitting hairs on a definition is not worth while. Practically, it is convenient to say that when one opens the roof of the bursa and finds the cartilage of the joint exposed to view through a rent in the floor of the bursa, we are dealing with a complete rupture. If there is no communication at all or only a small hole in the base of the bursa, we would class the case as incomplete. Of course the persistence of a direct communication between the joint and the bursa, even if small, is a most important point, because it alters the mechanics, as indicated on the cover of this book. Yet the size of the hole is also important if it is large enough to permit erosion of the joint cartilage (Plate VII, Fig. 8) by friction on the acromion.
It seems to me highly probable that incomplete rupture is much more common than complete. Since I have only operated upon cases where very pronounced symptoms existed, I have naturally found many more instances of the complete form, but in my observations on the cadaver, or on living cases in the clinic, I have much more often found incomplete lesions. I have not kept a numerical account and therefore cannot give the exact number or even the proportion.
Dr. Akerson's statistics give the best measure we have, but are subject to the criticisms on page 65. Similar observations may be made by any one having access to autopsy material. Moreover, when the economic importance of this lesion is appreciated, and the principles of efficiency become applied to the practice of medicine, such observations must be made.
I am inclined to think the table on page 469 also gives a low proportion of the incomplete ruptures, because so many cases in the other classes probably had this lesion besides the lesion which caused their classification. For instance, rupture of the supraspinatus is a not uncommon complication of dislocation and of circumflex paralysis, and many of the minor unclassified cases may have also been instances of this lesion. On the other hand, I have usually found at operation that the rupture was more extensive than I had previously thought, so that a good proportion of the supposed incomplete type may have been complete.
Referring to the chapter on Pathology, it will be seen that incomplete ruptures of four kinds are described:
(a) A few of the lower fibers on the joint side, together with the synovial reflection, may be torn out; these I call "rim rents."
(b) Some of the central fibers may be parted without tearing either the joint side or the bursal side of the tendon.
(c) The rupture may extend vertically through the whole tendon, making a communication between the joint and the bursa, without involving the whole breadth of the tendon.
(d) The fibers on the bursal side may be eroded without complete communication with the joint.
I believe that type (a) is synonymous with the cases so frequently found at autopsy where the sulcus is bare and eburnated, i.e., the condition I speak of as "rim rents." I think that type (b) may be the precursor of calcified deposits. Types (c) and (d) may be among the cases which give "tendinitis" symptoms out of proportion to the traumatic history.
Since I do not intentionally operate on incomplete ruptures, what I have to say in regard to these minor lesions is more theoretic than what has been stated concerning the complete ruptures.
All four varieties should be distinguished from the complete form by the persistence of considerable power in elevation, because the mechanics of the pull of the supraspinatus are not greatly altered. I have not operated unless there was decided loss of power.
The other cardinal symptoms, jog, crepitus, atrophy, sulcus, eminence and local tenderness, will be present, although any one of them or all of them may be found in less pronounced degree than in the complete cases. Type (c) might be recognizable, as the fluid sign should be present because joint and bursa communicate.
The diagnosis of the incomplete type is therefore made chiefly by the persistence of a considerable amount of power in the elevated or abducted arm and some doubt about the presence of some of the other symptoms and signs. Complete cases are usually so absolutely typical that no doubt remains. Complete cases do not form adhesions, while many incomplete cases do.
If the surgeon is sufficiently informed about the anatomy, pathology and surgery of this particular region, I believe that when in doubt he should explore the bursa through a half-inch incision. If he finds a communication through into the joint, let him close it, but if no opening exists, let him back out, for we do not yet know what to do to these incomplete ruptures.
Before closing this chapter, I may say that I believe these lesions to be the most common form of shoulder injury. My slogan has been that complete rupture of the supraspinatus is the most common cause of prolonged disability from industrial accidents to the shoulder. I feel that I have proved this at least to my own satisfaction. I may now add that the incomplete form accounts for the majority of minor shoulder disabilities. This I have not proved, for I do not operate on these cases, but the frequent presence of broadened sulci found in any .series of autopsies in elderly people is convincing to me. The clinical examination of employees with sore shoulders often shows symptoms suggestive of this lesion. Possibly opaque fluid injected in the joints might confirm the diagnosis. I have not felt justified in doing this, for exploration seems to me quite as free from danger. I certainly should try this experiment on patients now if I had in mind some definite plan for relieving them, if I did find broadened sulci indicative of incomplete ruptures, but I do not yet conceive of a plan by which to promptly cure them.
The appearance that I think opaque fluid in the joint would show in cases of complete rupture is indicated in the cover design.
----------------------------------------------------------
FREQUENCY OF COMPLETE RUPTURE OF THE SUPRASPINATUS TENDON
There are certain reasons for believing that this is a far more common lesion than is generally appreciated.
1. The writer's personal experience.
2. The statistics of Dr. Akerson.
3. The lack of attention paid to lesions of the shoulder in general; i.e., of end result studies of large series of shoulder injuries.
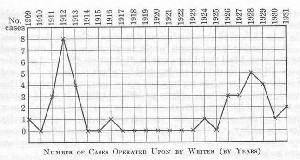
1. Personal Experience. The above chart shows that the writer's experience in operating upon these lesions was confined to two periods of about three years each, when attentive study was given to relatively large groups of shoulder cases. In the first period (1911 to 1913 inclusive) an intensive study was made of the shoulder cases at the Massachusetts General Hospital. The author resigned from that hospital in 1914 and was not reappointed until 1929. Other activities and a period in the army during the war intervened, without opportunity to operate on such cases, although I continued to make occasional impartial examinations for the Industrial Accident Board. In 1926, owing to the interest of Dr. Henry C. Marble and Dr. W. A. Bishop, who are directors of Insurance Clinics, I again gave intensive study to a group of shoulder cases, and the chart again ran to a peak. This led to increased interest in other clinics, so that other surgeons (e.g., Dr. Wilson) began doing these operations, which accounts for the decline at the end of my chart, although the rate of frequency, if we included other surgeons' cases, would not show this decline.
In other words, the chart shows that whenever I gave intensive study to a group of shoulder injuries, I was able to diagnose some of these cases and to demonstrate them by operation. My work received little attention after the first period but since the second, largely owing to the changes brought about by the Workmen's Compensation Laws, the importance of the lesion is becoming recognized by industrial surgeons in this state. I do not know just how many cases were seen during these two periods, and therefore cannot give the exact percentage of the cases examined which were instances of this lesion, although the limits may be stated pretty positively. For instance, the first fifteen cases were found among less than 200 patients, and the second fifteen cases were from an uncertain number, but probably less than 100. This means that the frequency of occurrence was about 7%% to 15% of all shoulder lesions that came under my observation.
By referring to my records for the twenty years since I recognized the first case, I find that I have seen in all about one thousand shoulder cases. Of these more than one hundred have been positively diagnosed as instances of complete rupture and many more as incomplete. This would justify an estimate of between 10% and 20%. It would require an amount of labor disproportionate to the present object to go over these records to apportion the exact percentage, since it is sufficiently clear that I have made this diagnosis in not less than 10% and perhaps more than 20% of all shoulder cases. If cases of partial rupture were included the percentage would be at least doubled.
The figures in the annual Reports of the Industrial Accident Board help us only in a negative way, for this diagnosis is not classified. Their tabulations of the durations of disability are not carried over from year to year, so that we cannot obtain a list of the cases in which disability is protracted. This is unfortunate, for this list would probably be largely composed of cases of rupture of the supraspinatus.
The report of the Industrial Accident Board for the year 1928, Table 7, gives the following figures in regard to shoulder injuries. It is supposed to cover every accident occurring in industry in this state.
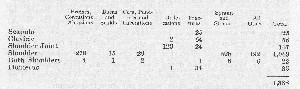
The last two columns, "Sprains and Strains," and "All Other," are the ones which would probably contain most of these ruptures, although a large number must be included under dislocations and fractures. If we double the figures where both shoulders were injured, the total of the two columns would be 748, five per cent of which would be thirty-seven. During the same period, July 1, 1927, to June 30, 1928, I personally made the diagnosis in seventeen cases which were referred to me by Insurance Clinics or by the Board for "Impartial Examination." Since I probably see but a small fraction of these shoulder injuries of doubtful diagnoses which occur annually in this state, the estimate of thirty-seven is surely a minimum one. The maximum reasonable estimate would double this and also include twenty-five per cent of the 125 dislocations. It seems to me pretty well proved that not less than thirty-seven and very likely more than one hundred injuries of this type occur annually among Massachusetts employees.
At first sight thirty-seven, or even a hundred, neglected shoulder injuries in a state of 4,200,000 inhabitants does not seem a very serious matter, but as each insured case may cost the state $4,000 for compensation (aside from the pain endured and the economic loss of productive effort in labor), the amount of money involved is considerable (37 X $4,000 = $148,000). This fact mates this obscure injury more interesting, and, if we multiply by 100, still more so. My opinion is that the larger figure is a more accurate estimate. If we included partial ruptures which heal after a few months, but which cause a large total of lost time, the annual expense to the state for injuries of this small tendon can be reasonably estimated to be over half a million. Furthermore, there must be many such injuries which are not industrial.
In addition to the above reasons for believing that this lesion is not rare, I may say that in a single set of twenty dissecting room subjects I have always been able to demonstrate one or more instances. When I have been asked to speak to small groups of doctors or students, I have usually been able to find a subject on whom to demonstrate the diagnostic signs of this lesion, by asking at adj acent clinics for cases complaining of inability to raise their arms. I feel quite confident that I can demonstrate (recognized or unrecognized) instances of this lesion by examination of the cases under treatment in the out-patient departments of any large general hospital in any city of the United States, and, in fact, probably in most parts in the world, where there are many persons over forty doing laboring work. This does not necessarily mean that there are large numbers, for each case is apt to be a patient for several years, meanwhile going from one hospital to another in search of relief.
2. Dr. Akerson's statistics, already given on page 67, give us a maximum estimate, because nearly all the observations were made on elderly subjects of the laboring class, in whom a previous injury could only be assumed, for there were no histories negative or positive of accidents. There is a splendid chance for a clinical research at the Long Island Hospital, in future, to correlate autopsy findings with retrospective histories of shoulder injury, taken from patients before death comes. It would be a time-consuming job, but it would help us to decide the important question of whether these lesions can occur without injury, and it might lead to the saving of many thousands of dollars, not only in compensation, cost of medical care and economic loss, but in maintenance of the indigent. Dr. Akerson's work might in this way lead to a saving of more than the cost of his entire department. Similar opportunities exist in like institutions from one end of the country to the other.
3. The Lack of Attention to Shoulder Injuries. There is a voluminous literature on fractures and dislocations (especially on habitual dislocations) of the shoulder, but, with the exception of Dr. Meyer's work (loc. cit.) and an investigation now being undertaken by Dr. Fowler of Evanston, 111., I know of no systematic observations from autopsy findings in this part of the body. Nor are there any serious studies of similar clinical cases. If the End Result system of organization existed in our hospitals and insurance clinics, these cases of prolonged disabilities would be automatically revealed, studied and eventually prevented by early operation.
Thus my confidence that these lesions are common is enhanced because no one has evidence to. contradict me, and a few support me. It is clear that Dr. Meyer finds similar lesions, although he explains them as the results of attrition. Dr. Fowler will, I believe, as he has already told me, confirm some of my findings and give support to those of Dr. Akerson.
ARGUMENT
This book is not written to show that I have had good results in this class of cases. My argument is merely that this lesion exists; is not uncommon; has characteristic symptoms which permit accurate diagnosis; and, since I have been able by suture of the tendons to greatly relieve a few cases, even though the diagnosis was belated, it is highly probable that the prolonged and trying symptoms from which these patients suffer, when not operated upon, might be prevented by early diagnosis and the prompt use of a minor surgical operation, which should not be difficult, if promptly done.
If I can offer reasonable evidence for the clauses italicized, it seems to me that the conclusions in the last clause of the above paragraph would be sustained sufficiently to justify prompt exploratory operation when the symptoms suggest this diagnosis.
POSSIBLE ACCURACY OF DIAGNOSIS
I have already established the existence of this lesion, endeavored to estimate its frequency and have described the characteristic symptoms. Evidence is now offered to sustain the statement that accurate diagnosis is possible. The following extracts, taken verbatim from my pre- and post-operative reports to insurance companies, show that a'positive diagnosis of this lesion may be made. Every case operated upon during the last sixteen years, in which I have demonstrated a complete rupture of the supraspinatus, is given. Even in the cases operated upon prior to 1916, one may find that my definite pre-opera-tive diagnoses in the records of the Massachusetts Hospital are correct, in all but five cases in which the diagnosis was simply " subacromial bursitis." With each of the abstracts given below the case number is stated. The reader will find further information about each of these cases by referring to these numbers in the Table on pages 255 to 260 in Chapter VIII.
CASE No. 57.
Preop. Diag. "The injury which he sustained two years ago, I believe to have been a rupture of the supraspinatus tendon and the upper portion of the capsule of the shoulder joint."
Op. Findings. "As soon as the bursa was opened it was apparent that the entire supraspinatus tendon had been torn away, for the cartilage of the bone showed where the supraspinatus tendon should be. A small stub of the tendon still remained attached to the tuberosity. Further exploration showed not only that the supraspinatus tendon, but the upper portion of the infraspinatus tendon was also torn, but the subscapularis was intact. The long tendon of the biceps could be seen crossing the field just at the edge of the subscapularis. The proximal portion of the supraspinatus had retracted so far into the subacromial space that only a rather unsatisfactory portion of it could be pulled upward and attached to the stub on the tuberosity. It was evident that the atrophy which had taken place in the two years left practically no hope of the restoration of the complete function of the muscle or tendon."
CASE NO. 75.
Preop. Diag. " I have no hesitation in making a diagnosis of rupture of the supraspinatus tendon, nor in advising an operation to suture it and clean off the ragged vegetations at the edges of the old rupture."
Op. Findings. " Showed supraspinatus entirely torn off and retracted far under acromion. Biceps tendon lying at inner edge of rupture."
CASE NO. 88.
Preop. Diag. "I feel that the diagnosis of subacromial bursitis is correct, but that the underlying cause of the bursitis was a ruptured supraspinatus tendon. This has now partially healed—enough to renew the power of abduction but not enough to make the point of rupture smooth. The result is an irregularity on the base of the bursa which in abduction impinges on the acromion and acromio-clavicular ligament."
Op. Findings. "On opening the bursa the ruptured supraspinatus tendon was beautifully demonstrated, the tendon having been torn from the tuberosity, leaving none of the original attachment on the bone. It had retracted about a half inch and the torn end could be seized with a tenaculum."
CASE NO. 88.
Preop. Drag. " He has the following signs indicating that his trouble is a ruptured supraspinatus tendon and his history is typical of this lesion.
"1. There is an acutely tender spot on the greater tuberosity at the normal point of insertion of this tendon.
"2. I can, I believe, feel at this point a sulcus where the tendon is torn.
"3. There is a painful jog in the motion as he raises his arm.
"4. There is velvety crepitus as he does this.
"5. After the arm has been elevated one can easily pull it down, although the deltoid muscle can be felt strongly contracted.
"6. There is a feeling of fullness under the upper part of the deltoid as if there was fluid in the bursa."
Op. Findings. "Free straw-colored fluid. Cartilage of head of humerus and the greatly swollen and injected biceps tendon visible on retracting the margins of wound in deltoid. The tear of the supraspinatus tendon was complete and the tendon of the infraspinatus was also almost completely torn. The proximal ends had retracted so as to be barely reached by Allis forceps to enable passing a suture."
CASE NO. 89.
Preop. Diag. "Patient presents to me typical symptoms of supraspinatus. He can abduct his arm slowly and with a hitch which gives an obvious sudden change in the relative position of the humerus and the scapula. He cannot maintain his arm extended against any considerable pressure."
Op. Findings. "Routine bursal incision disclosed a very extensive tear of the supraspinatus tendon. The biceps tendon had disappeared and could not be located except possibly as a few fibers in the anterior part of the joint."
CASE NO. 96.
Preop. Diag. "Examination shows pretty typical signs of a ruptured supraspinatus tendon, except that the friction rub is masked by the presence of joint fluid in the bursa. The outlines of the bursa are visible through a heavy deltoid as evidence of this fluid. It is well shown when the patient attempts to abduct the arm. The arc of abduction cannot be performed without a typical jog in the motion. The patient himself feels this and complains of pain during it. There is tenderness over the bursa."
Op. Findings. "Routine bursal incision showed a typical rupture of the supraspinatus tendon which did not involve either the subscapularis or the infraspinatus; making a gap pulled away from the tuberosity of about one-half inch width. Through this, on opening the bursa, the cartilage of the head of the humerus was visible. By retracting a little, the biceps tendon could be seen to the inner side, greatly congested."
CASE No. 97.
Preop. Diag. "Diagnosis. Rupture of supraspinatus tendon (left) complete and of severe grade. The same on right but incomplete and partially repaired. Probably rupture of the long heads of both biceps tendons."
Op. Findings. "The supraspinatus tendon was completely ruptured -and the upper portion of the subscapularis also. The biceps tendon had disappeared, evidently having been torn off the glenoid and retracted into its groove."
CASE No. 98.
Preop. Diag. "Examination shows very typical tenderness, crepitus, abduction weakness and the jog in motion typical of a ruptured supraspi-natus tendon in the right shoulder."
Op. Findings. "Routine bursal incision showed the supraspinatus was completely ruptured and also a part of the tendon of the subscapularis over the biceps tendon, and also a portion of the infraspinatus. The joint cartilage was exposed for about a half inch to the outer side of the bicipital groove and there was a tag of tendon still attached to the tuberosity just external to the groove."
CASE No. 102.
Preop. Diag. "Examination shows a decided atrophy of the muscles about the right shoulder, tenderness and irregularity of the tissue over the greater tuberosity, a painful jog in the motion of abduction, free external rotation, persistence of passive and loss of active complete abduction. These signs and the history are characteristic of rupture of the supraspinatus tendon. He also has' a rupture of the long head of the biceps, if one may judge by the contour of the belly of the muscle."
Op. Findings. "Free joint fluid found in bursa, which was large. The supraspinatus tendon was about half torn away from the tuberosity and the torn tendon retracted only about one-half inch, exposing a small extent (about) one-quarter inch of the edge of the joint cartilage. The opening was not large enough to view the tendon of the biceps, so I made an incision about one-half inch long into the bicipital groove and identified the biceps tendon. It was large and normal in appearance, so that it is likely that the apparent atrophy of the outer belly of the muscle in this case was due to simple disuse from reflex pain."
CASE NO. 106.
Preop. Diag. "Examination of the right shoulder shows typical signs of a rupture of the supraspinatus of considerable degree. One can feel the sulcus on the facet of insertion from which the tendon has been evulsed. There is fluid in the bursa."
Op. Findings. "The roof of the bursa was thickened. When incised, free straw-colored fluid escaped, about one dram. The supraspinatus was found torn from its attachment and retracted far under the acromion. About one-half of the insertion had evulsed from the facet. The other half was torn about one-half inch from the facet, leaving a thickened, irregular, whitish mass about the size of a large lima bean attached to the tuberosity."
CASE No. 107. Reported in text.
CASE No. 108.
Preop. Diag. "The diagnosis is fairly certain of a partial rupture of the supraspinatus, and also a rupture of the long head of the biceps."
Op. Findings. "The complete supraspinatus tendon had been torn close to the tuberosity and was retracted about an inch and a half. The infraspinatus and subscapularis were intact, but the biceps tendon had been torn completely off the glenoid and had retracted part way, instead of wholly into the sheath, leaving a frayed end protruding at the edge of the articular surface. In repairing I used this by sewing the supraspinatus to it and the subscapularis, anchoring the biceps tendon in its groove as I did so."
CASE No. 112.
Preop. Diag. "Examination shows the following: A slight atrophy of the intrinsic muscles of the shoulder, a soft crepitus which occurs with a snap just as the tuberosity passes under the acromion in abduction, a tender point on the greater tuberosity at the insertion of the supraspinatus tendon, a tendency of the scapula to follow the motions of the humerus, a flaccid condition of the outer head of the biceps muscle. These signs indicate that he has torn the supraspinatus tendon from its attachment on the tuberosity, and probably has also torn the biceps tendon from its adjustment on the glenoid."
Op. Findings. "This displayed a perfectly typical complete rupture of the supraspinatus tendon without rupture of either the subscapularis or infraspinatus. The biceps tendon was slightly frayed at its inner edge where there were two small papilloma-Iike, whitish excrescences, the size of one-quarter of a pea. The stub of the ruptured tendon was still attached to the tuberosity, but had worn down to a falciform edge; similar falciform edges showed on the lateral aspect of the tear; i.e., the unruptured edges of the subscapularis and infraspinatus. By lifting the edge towards the subscapularis, a pinkish, inflamed biceps tendon was demonstrated. A few fibers of the outer portion of this had been ruptured as spoken of before. There was only a moderate amount of joint fluid seen at any time. The edges of the torn surfaces were refreshed, and the parts sutured in place with three heavy braided silk sutures."
CASE No. 115. See history on page 389
CASE No. 119.
Preop. Diag. "Typical ruptured supraspinatus tendon. Atrophy, crepitus, jog, fluid, loss of power very great. Biceps O. K. Rotation free, tender sulcus."
Op. Findings. " The tendon was much thicker than usual and less retracted, so that the triangular gap was longer transversely than vertically. . . . There was quite a stub on the tuberosity, enough to suture. The biceps tendon was so badly damaged that there were but a few strands of it left and these were adherent to the roof of the joint. Most of the tendon had retracted into the groove and become adherent there. None was left crossing the joint surface and none was seen in the joint, although it might have been imbedded there behind the head."
CASE No. 123.
Preop. Diag. " This patient has the typical symptoms of a rupture of the supraspinatus tendon of considerable extent, but not enough to prevent his having a fair amount of power in abduction—although with pain. He has atrophy of the spinati, scapulo-humeral spasm, a j og in the motion of abduction, the fluid sign with limitation in complete abduction, a tender, palpable defect on the greater tuberosity where the tendon should be attached."
Op. Findings. "An exploratory incision a half inch long was first made and it was at once apparent that the supraspinatus and the infraspinatus tendons were evulsed from their facets, leaving no stubs of tendon. The biceps tendon, which was double at this point, was greatly swollen and inflamed and presented as soon as the roof of the bursa was opened. To its inner side the subscapularis and the inner portion of the tendinous expansion of all the tendons lay intact, and to its outer side was bare joint cartilage and the top and posterior portion of the greater tuberosity from which the tendons had been torn. The facets were smooth and the superficial parts of them had not been carried away by the tendons. The incision was enlarged to an inch and a half and a good view of the field obtained. It was found that the teres minor had also been evulsed. The whole posterior part of the capsule and conjoined tendon of the above muscles was retracted downward and outward. It was impossible to draw this back and to suture it in place."
CASE No. 127.
Preop. Diag. "At my first examination I did not make the diagnosis in this case, although it had been suggested by Dr. Marble, but on my second
examination, seventeen days later, I wrote, 'H--- is better, but I have
changed my opinion about the diagnosis. I am now quite confident that he has a ruptured tendon and should be operated upon. I think Dr. Marble was correct in his original diagnosis.' "
Op. Findings. "A small exploratory incision was first made over the point of tenderness. As soon as the roof of the bursa was incised, an irregular, whitish mass of tendon about as large as a thumb nail popped out of the incision. It proved to be the proximal portion of the torn tendon and was about one-quarter inch thick. It evidently turned on itself as the arm was abducted and caused the catch which the patient himself could accurately localize, There was about a tablespoonful of straw-colored fluid in the bursa. The incision was then enlarged to about two inches and a good view of the lesion obtained. This case differed from others on which I have operated in that the tear did not involve the whole thickness of the tendon, but left a very thin layer toward the joint surface so that there was not a demonstrable communication with the true joint. However, the layer was so thin that the cartilage could be seen through it. The ruptured portion formed a little flap about a square inch in extent, attached only to the proximal end and evulsed on the distal end from the facet of insertion. I have seen similar cases in the cadaver where the distal end had not evulsed. It is a fact that lamination of the tendon is found in many cases, but this is the first one on which I have operated where the laminated portion evulsed without the lower surface also tearing. The free portion seemed rather necrotic but was clearly rather recently ruptured. The torn surface was rather bulbous, as if partially healed. Near the lesion and to its inner side was a streaked, red area which was excessively tender when touched, but the torn end itself had no sensation and was not so made by the novo-caine. It is to be assumed, therefore, that the pain in these cases is not due to the tissue pinched but to the uninjured tissue on the tuberosity which does the pinching."
CASE No. 128.
Preop. Diag. " My opinion is very strong that he has a ruptured supraspinatus, but I am a little uncertain as to whether it is not a renewed injury in an old lesion. X-ray is very strong evidence of this. Clinically, I should not suspect it. In either case I should advise immediate operation as soon as arrangements can be made."
Op. Findings. "On opening the bursa there was found to be evidence of old inflammation in the bursa, as well as recent light adhesions. The supraspinatus was torn away from the tuberosity to the extent of about one-half inch, and little of the bursal floor remained untorn, but there was a gap directly into the joint through which the cartilage could be seen. This gap was about one-quarter of an inch in extent. The tendon had retracted very little and I was able to close it with four silk sutures, two of heavy silk and two of light silk."
CASE No. 129.
Preop. Diag. "Signs of ruptured supraspinatus tendon were present at my previous examination, but they are much more prominent now than they were at that time. He has a very distinct crepitus, sulcus, eminence, scapulo-humeral spasm, tenderness at the border of the tuberosity; localized tenderness, atrophy of the supraspinatus, sign of fluid when both arms are elevated. I agree with Dr. Marble in the diagnosis and would advise operation in this man's case."
Op. Findings. "The bursa was first opened by a half-inch exploratory incision. A small amount of free fluid escaped and it was readily seen that the supraspinatus tendon was ruptured and greatly retracted. . . . The tendon was partly evulsed and partly ruptured at the 'palisade junction.' The complete tendon was involved with possibly some of the infraspinatus. As in another recent case (H--- ) there was still some tissue remaining
on the joint side so that the cartilage was partly covered with a turgid, deep-red, softish tissue containing a few obvious whitish tendinous bands. One of these was especially noteworthy because it was very sensitive, and the patient winced when it was touched. I excised it because it did not seem to be of sufficient strength to make up for its sensitiveness. The biceps tendon lay to the inner side of the rupture buried in inflamed synovial folds, but not injured, unless the strand of tendon above alluded to had been stripped off it. The bulk of the proximal end of the supraspinatus tendon had retracted far under the acromion and could barely be drawn into the field."
CASE NO. 135.
Preop. Diag. " I feel very confident that he has a rupture of the supraspinatus tendon. I am not sure that there was not a previous rupture and that this latter accident merely increased the trouble. However, there is no question in my mind but that his chances will be much better if his bursa is explored and suture is done, if the tendon is ruptured."
Op. Findings. "No blood or fluid on opening bursa. A complete rupture of the supraspinatus, with extension across the bicipital groove, about one-half inch into the subscapularis. Definite indications that the rupture was fairly recent; i.e., very little separation between the distal and proximal portions. Stub of tendon still attached to the tuberosity over most of its extent. No new-formed falciform edge. Biceps tendon flattened and superficially reddened in portions beneath rupture. Parts satisfactorily sutured together with pedicle silk; five stitches. In my opinion, the condition found indicated a recent rupture of a tendon which had already been partially ruptured."
CASE No. 137.
Preop. Diag. "Examination shows that this patient has a symptomless, chronic bursitis, with crepitus in the right shoulder. The left shoulder shows the typical signs and symptoms of a rupture of the supraspinatus tendon. Since he has considerable power in abduction—although the abduction is painful, and accompanied with a jog and crepitus—I am inclined to think that the rupture is not extensive enough to involve the adjoining tendons. Even though this man is sixty-two, and it is four months since the injury, I would advise him to have the tendon sutured to the tuberosity."
Op. Findings. "A one-half inch exploratory incision was made and the bursa opened. Rupture of the supraspinatus throughout its whole extent was disclosed. The rupture extended also, to a slight extent, into the insertion of the infraspinatus. The sulcus and tuberosity were bare, except for a very slight amount of tag of tendon near the edge of the bicipital groove. The incision was enlarged to two and one-half inches to permit suture."
ERRORS IN DIAGNOSIS
But a skeptical reader may now ask for a statement of how many cases I have operated upon under this diagnosis and have failed to find a complete rupture of the tendon. I give below a similar set of verbatim extracts from the records of nine cases during the same sixteen years, the only ones in which I have made a positive diagnosis and have not been confirmed by the operative findings.
CASE No. 76.
Preop. Diag. "I believe this patient has a ruptured supraspinatus tendon, at the point of the insertion of the tendon in the tuberosity. This diagnosis is consistent with the X-ray appearances seen in the films taken by Dr. George. These films show an irregular opacity in the area of the bursa, which may be due to extravasated blood or to crumbs of bone torn off the tuberosity."
Op. Findings. The operative notes in this case have been lost, but I clearly remember that the condition proved to be a case of calcified deposit which had recently ruptured into the bursa, leaving a defect in the tendon very similar to a true rupture, but containing blood and calcified material.
CASE NO. 80.
Preop. Diag. "This is unquestionably a case of ruptured supraspinatus tendon of considerable extent, but the main symptoms are due to a tuft of synovial granulations from the remnant of the supraspinatus tendon still attached to the tuberosity."
Op. Findings. " The walls were much thickened and there were synovial tags in the region, over the tuberosity, showing more or less chronic inflammation. The tender point, which could be felt prior to the operation and was thought to be a tag of tendon remaining on the tuberosity, proved to be a rounded elevation, markedly circumscribed and about one-half inch in diameter, slightly longer in the axial direction than the transverse. This was acutely tender when pressed on. It was incised and found to be the insertion of the tendon of the supraspinatus attached to an osteophyte at the edge of the joint cartilage. There was no direct evidence of a rupture of the supraspinatus tendon. If there had been one, it must have healed. No communication with the joint was demonstrated. The essential pathology was probably the hypertrophic arthritis which was evident in other joints. (Patient's age was 77.)"
CASE NO. 91.
Preop. Diag. "The history and symptoms are typical of a ruptured supraspinatus tendon in the right shoulder, with some adhesions of the bursa, or blocking of the motion by the remains of the torn tendon impinging on the acromion. I think the latter."
Op. Findings. "The base of the bursa was deeply congested and swollen, but there was no demonstrable tear of the tendon of the supraspinatus. There were light adhesions in the bursa which were broken up with the finger. The short rotators and capsule were greatly contracted and were slowly stretched until full external rotation and abduction could be attained, and the wound closed."
CASE No. 105.
Preop. Diag. " I have little doubt that this patient has a rupture of the supraspinatus tendon of considerable extent."
Op. Findings. " Incision through the roof of bursa with the escape of about one dram of clear, straw-colored fluid. Exploration revealed an intensely inflamed zone on the greater tuberosity, approximately the size of a half dollar with red periphery and white center, resembling the condition seen in calcified cases. An inflamed fold moved back and forth over this as the patient's arm was moved. This fold was excised. The point of the knife was used to puncture the tendon in several places in the inflamed area with the purpose of allowing a new blood supply by attaching the scar to the inflamed base. There was no indication that the supraspinatus tendon had been ruptured."
CASE No. 110.
Preop. Diag. "The whole tuberosity is tender and it is hard to find a definite spot from which one can say the tendon has been torn. With the exception of this, his symptoms are fairly characteristic of a ruptured supraspinatus. From the relaxed condition of the biceps muscle and particularly of its outer head, I am inclined to feel that the biceps tendon is torn from its attachment on the glenoid. Indeed this may be the main lesion.
"I should advise inspection of his bursa under local anaesthesia and suture of the tendons if they are found torn. If there is no tear in the base of the bursa, I should advise opening the joint between the supraspinatus and the subscapularis and inspecting the tendon of the biceps.
"Remarks. This case is atypical in the age of the patient (17). Ruptured supraspinatus lesions are usually in elderly men. The character of the accident is unusual; sudden abduction efforts are more common as causes. There has been comparatively little pain, especially in the first week, and usually one has a history of swelling over the bursa in the first few days. Palpation over the tuberosity is a little atypical. For these reasons I cannot be as positive as I sometimes am, but I am sufficiently certain of a rupture to feel that in the boy's place I would want to have an exploration. Little harm would be done if this is negative, which I am confident it will not be."
Op. Findings. "The exploratory instrument was first introduced into the bursa, which was found to be full of adhesions and consisted of a series of pockets of walled synovia. Through the exploratory instrument it could be definitely determined that the bursa had been subacutely inflamed, but that there was no tear in the supraspinatus tendon. There was no fluid in the bursa. As both Dr. Baker and I thought that the biceps tendon was probably torn, the incision was enlarged to about one and a half inches, and the bicipital groove was incised. It did not contain the tendon, which evidently had retracted downward. The arm was put through the accustomed motions of rotation and abduction while a finger was introduced into the bursa to break up all the adhesions existing there. When the adhesions had been broken, which was easily done, the motion of the arm was normal. No steps were taken to repair the biceps tendon."
CASE No. 111.
Preop. Diag. "The shoulder presents typical signs of a ruptured supraspinatus tendon of a considerable degree. He has my fluid sign— characteristic velvety crepitus, a jog in motion, a tender irregularity on the greater tuberosity and weakness in abduction. He is able, however, with a little coaxing, to abduct the arm, but has very irregular action of the humerus on the scapula as he does this. There is still some ecchymosis in the anterior portion of the arm over the bicipital region, as if after the injury blood may have escaped down the tendon sheath; the tendon, however, appears to be intact."
Op. Findings. "Exploration of the bursa showed no fluid. No communication was found between the bursa and the joint. The bursa was adherent over about half the extent of the lower portion. On separating the adhesions it was evident that the supraspinatus had been torn, but had spontaneously healed; the tissues were red and swollen with white patches here and there. I therefore closed the wound in the usual manner without doing anything in the way of an operation."
CASE No. 120.
Preop. Diag. "The left shoulder presents very typical signs of an extensive rupture of the supraspinatus and possibly of the long head of the biceps. There is slight but decided atrophy—consistent with a history of two weeks. There is a very tender point on the tuberosity, scapulo-humeral spasm, a j og in motion and the fluid sign. In the stooping position the patient can abduct and hold the arm abducted as he straightens up."
Op. Findings. "Routine bursal incision. Adhesions prevented easy access, for roof was stuck to base over an area as large as a quarter over the greater tuberosity. These were separated and showed that the tendon of the supraspinatus was bright red, swollen, and covered with tags of vascular adhesions. The line of demarcation of the affected area was very sharp on the outer side, so that the contrast between the yellowish white to the right and the turgid red at the left was very decided. It suggested an infarction. Although there was some free fluid in the bursa there was no communication through the inflamed area to the joint. The supraspinatus tendon, if ruptured at all, must have been torn beneath the base of the bursa without communicating with the bursa. Several small incisions were made with the point of the knife to relieve tension in the tendon. Through one of these a tiny bit of white nondescript tissue protruded. This was saved for pathologic examination j I am pretty sure it was necrotic tendinous substance. The wound was closed as usual without endeavoring to suture the roof of the bursa. The pathology found at this operation may be explained in two ways, or as a combination of both ways. There was certainly an acute bursitis with recent adhesions, but it was impossible for me to say positively that this localized acute inflammation over the site of the supraspinatus tendon was due to a rupture of the tendon beneath the base of the bursa. It might have been due, as suggested by the evidence of osteitis shown in the X-ray, to a chronic necrotic process in the tendon. The extrusion of the bit of necrosed tendon from the incision also supports this. So does the symptomless condition in the well shoulder. It seems to me that if we accept the man's history that the condition of the shoulder was O. K. before he helped lift the case, that the whole picture can be explained by the supposition that there was a necrotic process going on in the tendon which had weakened it so that it partially evulsed without tearing into the bursa. This would explain all which was found at the operation, and my opinion is that this theory truly does account for the facts. I have had several other similar cases and have frequently seen evidence of such lesions in the cadaver."
CASE No. 126.
Preop. Diag. August 12, 1929. "I have little doubt that this patient has a mild rupture of the supraspinatus, but as the power in abduction is good, operation need not be considered. It is probably not an extensive rent. I suspect both from the clinical signs and from the X-ray that he has had an old lesion here for some years. It seems to me that the best plan of treatment would be to let him rest a few weeks and to have him attend your clinic three times a week for massage. If he does not feel able to go to work again in a month, let me see him again." Sept. 22, 1929. "Examination is as on August 19th. My opinion that he has a small rupture of the supraspinatus is somewhat strengthened by the fact that the symptoms have not improved. As he is only forty-two, I am inclined to advise an exploratory incision under novoeaine to confirm the diagnosis and, if necessary, to suture the tendon. The spot at which he complains of tenderness is so localized that it seems likely we shall find some lesion at this region."
Op. Findings. Oct. 23, 1929. "Under local ansesthesia no rupture of the tendon was demonstrated. The walls of the subacromial bursa were thickened and the bursa contained a little fluid. There was nothing found which indicated any recent injury other than the presence of this chronic bursitis. The wound was closed after taking out a small specimen of the synovial lining for pathologic examination." (This showed chronic inflammation.)
CASE NO. 181.
Preop. Diag. "In my opinion, he has a chronic subacromial bursitis in consequence of a rupture of the tendon of the supraspinatus."
Op. Findings. "A half-inch exploratory incision showed that the roof of the bursa was thickened and adherent to the floor beneath. The wound was enlarged to about one and one-half inches and the adhesions freed, partly by cutting and partly by tearing with the finger. Several small bursal sacs had replaced the usual large one. These sacs lay beneath the adhesions which permitted a certain amount of motion. The adhesions were red and inflamed looking. There were one or two small calcified deposits which were wiped out. The periphery of the bursa outward and backward under the acromion was more normal in appearance and not adherent. The total area involved by the adhesions was about the size and shape of a fifty-cent piece over the greater tuberosity and insertion of the supraspinatus tendon. The most acute tenderness was felt at this point, although there was a little sensitiveness over the bicipital groove. Two or three tags of inflamed serosa were removed for examination and a very small bit of tendon at the point where the adhesions centered was clipped out for examination."
In most of these nine cases, although there was not a complete rupture, there was some evidence of partial rupture beneath the base of the bursa. However, I did not confirm this supposition by cutting through the base, for it seemed to me that its tissue formed a bridge over the gap which would assist in healing the tendon. I am inclined now to think that I have been too conservative, for several of these cases had long convalescences, and it might have been wiser to explore beneath the base of the bursa.
At the danger of repetition, I wish to state that I do not intentionally operate, unless I think the ruptures are complete, because I feel confident that where the rupture is complete, healing will not take place unless suture is done. I am not sure enough of what the treatment of partial ruptures should be, to make me urge operation, even if I were sure of the diagnosis. Therefore, the above nine cases may be considered to be errors in diagnosis, although by no means as negative explorations. The difficulty is to tell beforehand whether or not there is actually a complete rupture which needs suture. I think the fact that during a period of sixteen years I made the diagnosis correctly twenty-one times, and incorrectly in only nine cases, shows that the diagnosis is not difficult. When in doubt, such a trivial operation as exploration would be justified, even if the proportion of errors was three to one.
In several of the nine cases it is to be noted that the mistake could have been avoided by more reliance on the fact that if there are decided restricting adhesions the diagnosis is not established. In the first case the X-ray indicated the presence of a calcified deposit and should have warned me not to make the mistake, although I should have operated at any rate. In several of the other cases where a mistake was made, the notes indicate that I was in decided doubt about the diagnosis before the operation, and, therefore, the incision as a matter of fact was "exploratory."
END RESULTS IN OPERATED CASES
We next come to the clause "since I have been able to relieve a few cases even though the diagnosis was belated." By referring to pp. 255-260, the reader may see that, excluding cases where there was a coincident fracture of considerable extent, I have operated on thirty-seven cases. In four of these the tendon was retracted to such a degree that I could not even attempt a suture. I have been unable to trace two patients operated upon about twenty years ago. Deducting these six cases we have thirty-one in which an attempt was made to suture the tendon. The results have been as follows: poor, four; fair, seven; good, twenty. That is, two out of every three operations were successful in that the results enabled the patients to return to work, although in most cases only after the elapse of months.
A very few, but not many, of my results have been perfect in the sense that the arm was just as useful and just as painless as before the injury; but many of them have been good in the sense that the arms have been relatively painless and quite, if not completely, useful. When I have written "good" I mean that the operation was well worth doing. When I have written "fair" it should convey that, in my opinion, there was some improvement from the operation, but that it was hardly worth doing. "Poor" means that the sum total of relief of the suffering of the patient was not sufficient to compensate for the pain and trouble which were incident to the recovery. There have been no bad results in the sense that any joint was made worse by the operation, but in at least two of the "fair" cases (Cases 83 and 112, see p. 175) the patient's point of view would have been that the result was poor, because his symptoms were not improved in spite of his post-operative pain.
There are many factors to account for the lack of perfection in the results, such as the age, the length of time the operation has been delayed, coincident disease, and above all, the desire of the patient to get well. The non-industrial patient is more readily pleased by improvement which lacks perfection than is the employee, who prefers compensation and no work, to double the pay plus work which would undoubtedly cause some pain and discomfort.
This compensation factor always causes some delay in the convalescence. Hard times have the same effect.
However, my argument does not need to show that all results should be perfect. I could give many excuses for the failures, but will be contented to present the following table.
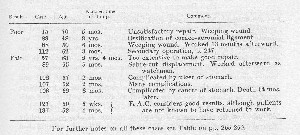
In three of the four poor results, the tear was very extensive and the repair unsatisfactory; three had weeping wounds from excessive fluid drainage without frank sepsis (see p. 248), and all four had secondary operations. The seven cases of fair results were all improved to a considerable extent but have not actually gone to work again permanently.
There was one death which might possibly be attributed to the operation. This patient, Case No. 123, was drowned while in bathing at one of the beaches three weeks after I did an exploratory operation. The operation had shown that the tendons were too badly injured to admit of any attempt at repair. The wound healed by first intention, and as the patient enjoyed going in bathing I permitted him to do so about ten days after the operation. On the twenty-first day he was drowned. He was known to have had a heart lesion. The medical examiner reported "Death by drowning," and did no autopsy. I myself can see no connection between the operation and the drowning, but two doctors offered testimony at the Industrial Accident Board that the patient had had pulmonary embolism from the operative wound. The Board, however, did not accept their testimony, because there was no autopsy or other reason to support their diagnosis.
I feel that the proportion of good results is a sufficient reason for advising this operation, even in late cases. With greater experience and improved technique it is likely that the percentage of good results will be increased, but, as in many other surgical conditions, prompt recognition and treatment will be of greater importance than the difference in surgical skill between experienced and inexperienced operators, provided the pathologic condition is thoroughly understood.
END RESULTS IN UNOPERATED CASES
As most of my cases have been "industrial" the question of compensation becomes an important factor in estimating the period of disability. Cases who have no prospect of compensation will unquestionably go to work sooner; for instance, Case 119, a painter who had his own shop, began doing some work within a month after his operation. On the other hand in some cases, the compensation becomes equivalent to an old age pension. I have spent much time and money in tracing the unoperatcd cases of both partial and complete rupture, and have obtained enough information to venture the estimates on page 124 as to the probable costs of each. My estimate of $300,000.00 for 100 cases of complete rupture is also sustained by figures on ten patients on whom I did operate and therefore established the diagnosis. In five of these (delayed) cases the operation was a practical failure, but the patients were no worse off in consequence, and therefore were in a similar status to those in which no operation was done. In the other five the operation was essentially successful.
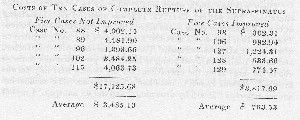
(The law limits total compensation to $1,000 so that these figures do not cover the period the patient is still disabled after his compensation ceases. The figures also include all medical and surgical charges.)
Case 96 in the first group had a delayed convalescence but eventually was able to go to work again as a steamfitter. Case 127 in the second group was a similar one. The reader may shift either case to the other group if he is disposed to exaggerate either average figure. Although it would not be fair to use the second group at all in computing the cost of 100 unoperated cases, by using it we may obtain an average minimum figure — $2,143.00. Therefore, the figure for 100 cases must be somewherebetween$200,000.00and$4-00,000.00.
Pain and disability are difficult to estimate in figures; these estimates are presented to impress on the reader that this lesion is important.
REFERENCES
BTTCHOLZ, C. H., Der Abriss der Supraspinatusshue, Arch. f. klin. Chir., Berlin, 1922, cxxi, 255-264.
CODMAN, E. A., Abduction of the Shoulder. An interesting observation in connection with Subacromial Bursitis and Rupture of the Supraspinatus, Boston Med. and Surg. Jour., 1912, clxvi, no. 24, 890-891; Also: Complete Rupture of the Supraspinatus Tendon. Operative Treatment with Report of Two Successful Cases, Boston Med. and Surg. Jour., 1911, clxiv, no. 20, 708-710; On Stiff and Painful Shoulders, As Explained by Subacromial Bursitis and Partial Rupture of the Tendon of the Supraspinatus, Boston Med. and Surg. Jour., 1911, clxv, no. 4, 115-120; The Pathology and Treatment of Lesions in and about the Shoulder Joint. The Industrial Doctor, 1926, iv, No. 8,121-131; Obscure Lesions of the Shoulder; Rupture of the Supraspinatus Tendon, Boston Med. and Surg. Jour., 1927, cxcvi, no. 10, 381-387.
FOWLER, E. B., Rupture of Spinati Tendons and Capsule repaired by new operation, Illinois M. J., 1932, lxi, 332-334.
KITCHEN, A. S., Surgery of the Supraspinatus Muscle, Journ. Michigan M. Soc,
1920, xix, 64-67.
METER, A. W., Absence of the Tendon of the Long Head of the Biceps. Jour. Anat. and Phys., 1913-1914, xlviii; Also: Anatomical Specimens of Unusual Clinical Interest, Am. J. Orthop. Surg., 1915, xiii, 86; Unrecognized Occupational Destruction of the Tendon of the Long Head of the Biceps Brachii, Arch. Surg.,
1921, ii, p. 130; Further Observations Upon Use-Destruction in Joints, Jour. Bone and Joint Surg., 1922, iv, p. 491; Evidences of Attrition in the Human Body, Proc. Am. Assn. Anatomists, Anat. Rec, 1923, xxv, 142; Further Evidences of Attrition in the Human Body, Proc, Am. Assn. Anatomists, Anat. Rec, xxvii, 211, 1924; Further Evidences of Attrition in the Human Body, Am. Jour. Anat., 1924, xxxiv, 241; Spontaneous Dislocation of the Tendon of the Long Head of the Biceps Brachii, Arch, of Surg., 1926, xiii, 109; Spon
taneous Dislocation and Destruction of Tendon of Long Head of Biceps Brachii j Fifty-nine Instances, Arch, of Surg., 1928, xvii, no. 3, 493-506; The Minuter Anatomy of Attrition Lesions, Jour. Bone and Joint Surg., xiii, 841, 1931.
WARNER, F., Injury to Tendons and Joints, Intn. J. Surg., N. Y., 1918, xxxi, 196. WILSON, P. D., Complete Rupture of Supraspinatus Muscle. J. A. M. A., 1931, 483.
So far as I know there is at present no literature on the subject of this chapter which deserves serious study, except that comprised in the above references. I have no doubt that Doctor Meyer and I refer to the same lesions which were studied by Doctor Akerson and can be found by any one who wishes to look for them in similar material. Doctor Meyer's attention has been focused on the long head of the biceps; mine has been focused on the supraspinatus. Probably both of us are in a measure right, and in great measure wrong, but at least we have opened up the field for future students who wish to relieve persons incapacitated by lesions in this region of the body.
