
The role of the supraspinatus in dislocation...
CHAPTER IX
THE ROLE OF THE SUPRASPINATUS IN DISLOCATIONS AND FRACTURES OF THE SHOULDER JOINT
THIS chapter does not aim to be an exhaustive treatise on fractures and dislocations of the shoulder, although a very large number of articles have been studied in order to compile it. During the summer of 1928, Dr. T. W. Stevenson reviewed the literature for me, with especial effort to find to what extent the bursa and the short rotators had been referred to. At about the same time, I took advantage of the service of the Library Bureau of the American College of Surgeons, with the request that they find for me all the references they could concerning rupture of the supraspinatus tendon. After a careful search they were unable to find any articles whatever which were devoted to the subject, although occasionally they found references to rupture or avulsion of the tendons in cases of dislocation on which operations had been done.
So far as I know there is no record in the literature of what I call the "Pivotal- Paradox," described on page 43. I, myself, did not understand this paradox when I started to write the book, and only gradually puzzled out its meaning and significance. Certainly none of the authors, who have written on dislocations and fractures in this region, seem aware of the facts that in complete elevation of the arm almost no rotation can occur and that the extent of rotation diminishes as the arm is elevated. The lack of this knowledge of normal functions seems to me to render most of the previous explanations of the mechanism of dislocations and fractures in this region nearly worthless, for several important deductions can be made by the use of these facts. I have consequently eliminated much that I had previously written about the opinions of authorities.
In complete elevation there is only one possible geometric relation of the two units, i.e., the head of the humerus and its tuberosities, with the scapula and its processes. No matter in what degree of rotation you start to raise your arm and no matter in what plane you raise it, the capacity for rotation will be less and less as the arm ascends until, in complete elevation, tuberosities and processes will be locked in a fixed position. In this fixed position the articular head of the humerus will be shown by X-ray in the antero-posterior view, to face nearly outward, and in the lateral view to face somewhat forward, i.e., it actually faces obliquely outward and forward, exactly reversed from its anatomic position. The axis of the condyles of the lower end of the humerus becomes antero-posterior, with the internal condyle pointing forward. The humerus has rotated inward 90° and has become inverted. You may say that the angle between the shaft and the axis of the neck gained 45° by inversion and then 45° by external rotation, or you may say, if you please, it first gained 45° by internal rotation and then another 45° by inversion. Do not proceed with this chapter until you are sure that you have understood this paragraph, even if it is necessary for you to take a humerus in your hand.
The reader must bear in mind that this pivotal position may be assumed by extension of the scapula on the humerus as well as by extension of the humerus on the scapula. For instance, the arm may be in this position when a boxer delivers a telling punch, "putting his body into it." However, the true pivotal position implies that the clavicle is elevated and carried backward to its extreme limit when the arm is elevated to its extreme degree. In other words, the scapula and humerus may move into their share of the pivotal position without the clavicle rising (subordinate pivotal positions), but the arm, to attain complete elevation and the true pivotal position, must be raised to the side of the head.
The scapulo-humeral joint will lock in different positions according to the degree of rotation of the humerus, in a very queer way. (See Figs. 25 and 26.) There can be very little scapulo-humeral abduction with the humerus in full internal rotation; i.e., when the forearm is behind the back, even if clavicle is raised. Starting with your clavicle held down, try elevation of your arm in either internal or external rotation, and then compare the extent of motion when you start with it raised. You will see why authors have differed so much in their estimates of the degree of motion possible in the scapulohumeral joint. To get the maximum you must perform elevation in internal rotation in the sagittal plane or external rotation in the coronal plane; you cannot interchange. These motions cannot be estimated by putting the scapula of a cadaver in a vise, because in life they vary with the relative positions of humerus, scapula and clavicle.
It is as if the secondary humeral joint, limited by the acromion and coracoid, were built with two long sloping sides meeting at an angle above the head, so that when the arm is raised in any plane it eventually comes to rest in the trough formed at the angle of the coronal and sagittal planes and cannot rotate any more. Nature's command is: "Make any combination of elevation and rotation within this enclosure which you wish, but if you exceed these normal limits, you may dislocate or fracture your humerus."
A logical conclusion from these facts is that in whatever way a forward or lateral fall occurs, no strain will come on the scapulohumeral structures until they assume this locked position in complete elevation, provided rotation of the humerus is unhindered as the arm is being elevated. In other words, when the arm is being elevated in mid-rotation in the sagittal plane and arrives at a little above a horizontal position, if inward rotation be prevented, some structure must give, provided the fall continues in this plane. This is exactly reversed in the case of falls in the coronal plane, for when outward rotation is prevented, some break in bone or soft parts must occur. The latter example is the usual one in dislocation and fracture of the head of the humerus.
Let us imagine the same forces applied in another way, i.e., by leverage on the arm when the body is in a fixed position, for mechanically it is the same problem whether the falling patient exerts force on the outstretched arm, or the fixed patient has the same force applied to the arm. Let us imagine the arm thrust into a pipe and force applied to that pipe as in the following diagrams, by lifting its free end up from the plane of the paper- (Fig. 53.)
In making an effort to remember the combinations of rotation and elevation of the arm which may or may not be made, a simple formula is this: evolution has fitted the human animal to fall directly forward on his face with his arm and forearm in almost any position in relation to his body, but, once he has fallen, his arm and forearm cannot be brought much behind the plane of his body in the position in which he lies on his face on the ground, without in some way raising his body.
We may learn a good deal about the shoulder joint from watching the maneuvers of a wrestler endeavoring to turn his opponent from a face-downward position. These maneuvers are essentially the same as those represented in the diagrams above, that is, they depend on getting the flexed forearm in such a position that a little more leverage would break or dislocate the humerus, unless the prone wrestler does permit his body to be raised. Of all the possible positions in which his forearm and arm can be pulled backward, that in which the arm lies at the side will show the greatest backward mobility, i.e., "dorsal flexion."
In lateral falls, when the abducted arm is held behind the plane of the body, the same dislocating or breaking strains that the wrestler endeavors to secure may be produced, the force being supplied by gravity. Moreover, falls will be more violent and sudden, and perhaps catch the muscles when relaxed, instead of having the opposing muscles offer resistance by the voluntary tension which the prone wrestler can assume.
.jpg)
FIGURE 53. LEVERAGES CAUSING ANTERIOR AND POSTERIOR DISLOCATIONS
In interpreting this plate the reader must imagine the arm thrust into a pipe, and he must suppose that the patient's body remains in ironlike rigidity while the outer end of the pipe is raised directly upward from the plane of the paper. Provided the body remained rigid and the tube were raised in this manner, a dislocation of the head of the humerus or fracture must occur. Typical backward or subacromial dislocation would occur in Figures 2, 6 and 7, while subcoracoid dislocation would occur in the other positions.
As in simple frontal falls, so in simple dorsal falls no dislocation of the shoulder will occur, if the arms are free, for we may lie on our backs with our arms in any position anterior to the coronal plane of the body. Even when the dorsal fall occurs with the forearm behind the back or behind the head, dislocation is unlikely.
Thus we reach the conclusion that only headlong, lateral, or semi-lateral, sudden falls can produce the forced elevation combined with prevention of rotation which is necessary to cause anterior luxation of the shoulder joint.
It is possible to conjecture, from a more detailed study of the questions just considered, which forms of dislocation, or varied locations of the lines of fracture, will occur in the shoulder if the lines of force are known. For instance, it is safe to say that only the results of forces applied as in Cuts 2, 6 and 7, in Fig. 53, may result in subacromial dislocation, while all of the others produce subglenoid dislocation.
To express the writer's belief in another way: anterior dislocations of the humeral head occur after the arm has reached the fixed "pivotal position," or more often by prevention of rotation when the arm is at least above the level of the shoulder and the extent of possible rotation therefore greatly diminished; subacromial displacements occur when the arm is below the level of the shoulder and is rotated internally.
This belief is founded not only on the facts already mentioned, but on two others. The first is the remarkable ability of the arm to rotate quickly. Any one who has done any wrestling will remember how elusive were his opponent's arms, unless his elbows were bent, and how easily they slipped out of his grasp as he endeavored to obtain a "shoulder lock." The second is the utter unreliability of the histories given by patients of falls "on the shoulder." The reader is again referred to p. 10. Patients with these injuries almost always say that they struck their shoulders and do not realize that they fell with their arms elevated, i.e., raised to fend off the ground. The inertia of the body is so great as compared to that of the arm, that even in a sudden fall the arm may be thrust forward or outward before the body reaches the ground. A man must already be hugging something, as a football, under his arm in order to fall on his shoulder.
The fact that the arm rotates readily in a safe direction as it is instinctively raised (i.e., raised in relation to the scapula, although pointing downward) during a fall, means that subconsciously the arm will usually reach the relatively safe pivotal position. Meantime the palm meets the ground and the force becomes disseminated to the various ligaments, muscles and bones of hand, wrist, elbow, shoulder and back, each in turn breaking the fall until the final bony lock in the pivotal position brings the stress to a limit. Even then the pec-toralis, the teres major and latissimus, and finally the clavicle, may still further disseminate the stresses. But notice that in this elevated position the lines of force of these muscles converge toward the glenoid, so that they are not, in this position, functioning as rotators as they do when the arm is at the side. The higher the axis of the humerus the more their power is exerted toward the face of the glenoid in their effort to avert the leverage of the shaft from gaining a fulcrum on the acromial edge. However, while they are in use in fending off the ground, the pectoralis and latissimus are acting also as strong internal rotators. This is the period of danger (Fig. 55), for the pivotal position, once reached, means safety, unless the downward factor in the fall is great. When the arm is in the pivotal position, the broad tendon of the latissimus actually covers the unprotected axillary portion of the capsule and tends to prevent the head from dislocating, although the pull of this muscle is in the main downward. In this position the long head of the triceps, the teres major and the latissimus actually form a support for the lower half of the capsule.
.jpg)
FIGURE 54. ACTION OF PECTORALIS MAJOR IN DISLOCATION
This diagram pertains to the discussion of whether the pectoralis major and latissimus dorsi should be regarded as furnishing a fulcrum in case of fracture of the upper end of the humerus. The contention is made that the pull of these muscles not only does not act as a fulcrum, but to some extent relieves the strain on the surgical neck, by pulling the tuberosities away from the true fulcrum which is the acromion. If these muscles acted as a fulcrum, the power would be applied on the glenoid and would immediately rotate the whole scapula, so that the acromion would become a fulcrum. The writer holds that in such accidents there can be no disruptive force in the region of the head of the humerus unless the acromion does act as a fulcrum.
The diagram further illustrates the fact that the power of the supraspinatus is applied in such a manner as to restrain dislocation, but that in forced elevation of the arm the upper edge of the glenoid acts as a wedge driven in between two points of application of strain. This idea is amplified in Plate IX.
Many authors have contended that besides the obvious bony fulcrums which occur, there may be others momentarily maintained by contracted muscles, which may lead to fracture or dislocation. Perhaps this is true, but I have been able to work out few such mechanical positions. For instance, the lever formed by the humerus when the arm is in the anatomic position, the pectoralis and latis-simus contracted, and outward force applied at the elbow, may be considered either to have its fulcrum on the glenoid or to apply power there, with the pectoralis, etc., as a fulcrum. The latter might be the proper way to consider the problem if fracture occurred in the long arm of the lever, distal to these muscular attachments. It seems more logical to me to regard the applications of muscle pulls as forces acting on the obvious bony fulcrums. However, there can be no doubt that when these muscles are contracted they would tend to prevent outward rotation of the humerus.
.jpg)
FIGURE 55. TRAJECTORY OF CENTER OF GRAVITY
The center of gravity of a person in falling necessarily always has a trajectory formed by the momentum with which he falls forward, combined with that with which he falls downward, and that which is exerted in relation to the median plane. The writer contends that in most instances, dislocations and fractures in the region of the upper end of the humerus take place when the trajectory meets the ground at or posterior to the point of impaction of the elbow, and also internal to this point. If the trajectory came far anterior to the point of the elbow, the arm would be folded to the side, or if it came far posterior to the point of the elbow, the arm would extend harmlessly beside the head. If it came near the median plane or to the opposite side of it, the arm would slip outward into the hammock position. It therefore seems highly probable that most of these fractures happen when the arm is internally rotated by the pectoralis, etc., and the fall is of such a sudden and violent character that the humerus does not have time to rotate.
If the vertical factor in the trajectory were great so that the patient was falling nearly straight, head downward, fracture or dislocation in the pivotal position would occur. The writer believes that in every case there is acromio-humeral contact, and therefore always a subordinate pivotal position (see Fig. 25).
I am not in sympathy with the view of those authors who hold that the contracted pectoralis and latissimus act as a fulcrum to promote dislocation or fracture of the head of the humerus. I think the reverse is true, so far as their adductor action is concerned, for I am convinced that this action merely tends to prevent dislocation, since the force is applied to the long arm of the lever distal to the true fulcrum which is the acromion.
Lack of space prevents elaboration of the following additional reasons which support this conviction.
- The directions of the majority of the fibers of the pectoralis
major suggest that -their contraction would bring the head toward
the glenoid from the very start of elevation, i.e., they would directly
oppose dislocation.
In other words, the lower fibers of the pectoralis are inserted higher on the humerus than the upper fibers; thus all fibers of the muscle tend to pull in a line away from the acromion as a fulcrum while the arm is being raised. - The combined power of the adductors would not be enough to break the humerus, if both ends of the latter were fixed. Therefore, their power would not be enough to act as a fulcrum for a fracture in the short arm of the lever, although it might be sufficient in the long arm.
- Even if the power on the long arm of the lever'acting through the muscles as a fulcrum, became applied to the glenoid and to the supraspinatus and other opposing muscles, the result would merely tip the scapula so as to apply the acromion as a fulcrum.
- Until the acromion became a fulcrum no disruptive force could take place between the scapula and humerus.
- If the humerus touched the acromion at all and the pectoralis, etc., applied their power exactly opposite this point, the leverage exerted on the glenoid would not be changed in any way; nor would it be changed much if the point of application were moved a little away from the neutral point on the long arm of the lever. However, that slight change would diminish rather than enhance the tendency to dislocation.
- The X-ray shows close apposition of acromion and humerus, when the arms are akimbo, in the salute position and in complete elevation.
- The acromion is always the fulcrum, although in the above positions different parts of the acromial edge come in contact with different parts of the circumference of the humeral head. (Fig. 25.)
Although I believe that the pull of the pectoralis and latissimus actually help to prevent dislocation by their action as adductors, I am strongly of the opinion that as internal rotators they actually help to promote dislocation. The reasons may be briefly stated a& follows: On account of the position of insertions of their tendons, to be adductors, they first have to be internal rotators. As adductors they do their best to fend off the ground until the last possible moment when the acromion has begun to be a fulcrum. Meanwhile, as internal rotators, they are drawing the arm into a subordinate pivotal position and thus prevent external rotation, which is the only method of escape for the arm if it must rise in the coronal plane. Thus we can conceive of their having power enough to keep the humerus internally rotated until it is too late for it to turn, although we cannot conceive of their being able to act as direct adductors strongly enough to withstand the falling weight of the body. If, in any case, they instinctively relax in time for rotation to occur, the arm will rise to the side of the head and no harm will have been done. Occasionally, however, the relaxation is too late, or vice versa, the violence is too sudden, and the arm will be caught in internal rotation in or near the coronal plane. It will then be too late for the adductors to relax in order to let rotation occur and thus permit the arm to ascend by the head.
The nearer the bent arm, in internal rotation, lies to the sagittal plane the safer it will be; the nearer the externally rotated arm lies to the coronal plane the safer it will be and vice versa. As a matter of fact, in healthy youth it is astounding how rapidly this instinctive rotation will occur. The football player may be hurled headlong by impact with other players in such a way that his body may be twisting laterally as it falls, yet his outstretched arms fend off the ground just long enough to prevent his breaking his neck, and in spite of the sudden, twisting violence, rotation at the last moment usually avoids dislocation of the shoulder.
Yet occasionally the resultant of all the forces of the fall makes the trajectory of the center of gravity strike posterior to the point of the elbow and to its inner side, while the humerus is internally rotated, and anterior dislocation will occur.
If the reader wishes to go into this in more detail he may force his mind to project a combination of Figures 26 and 55. It is difficult enough to visualize the normal workings of the shoulder joint, but it is still more difficult to foretell the results, on this beautifully adjusted apparatus, of a fall downstairs. Yet I think these general principles usually apply.
On the supposition that our conclusion that the humerus must obtain a fulcrum on the acromion in order to exert a disruptive force to produce dislocation is correct, let us consider what occurs in the inner unit of the shoulder, Figure 8, Chapter I.
The fulcrum on the edge of the acromion obtains its skeletal support, whatever the position of the arm, directly through the clavicle to the sternum. As has been said, not only is upward dislocation of the acromio-clavicular joint prevented by the fact that the clavicular portion of it is superior, but by the strong coraco-clavicular ligaments. Thus the clavicle in any position furnishes a strong radius through which the pressure on the fulcrum is firmly sustained. Moreover, the S shape of the clavicle has been shown to not only withstand great pressure in a line between its two ends, but to have great elasticity when the pressure is released.
I wish to accent again three characteristics of the scapulohumeral joint.
- The capsule is necessarily loose.
- The upper half is muscular and strong; the lower half is fibrous and weak.
- Since the humerus can rotate many degrees (probably 100+) without moving the scapula, any one of the short rotators may receive the chief burden of the strain according to the degree of rotation when the acromion becomes the fulcrum. The following remarks will be based on the supposition that the supraspinatus is uppermost, as in Fig. 9, but would apply equally well when any of the other rotators were directly opposed to the force moving the elbow.
As the elbow rises upward not only is the supraspinatus contracted but the upper edge of the glenoid becomes a wedge in the reentrant angle, between the articular cartilage and inner surface of the supraspinatus. This accounts for the frequency with which fracture of the tuberosity accompanies dislocation. In most cases not only the facet on the tuberosity for the supraspinatus will be carried away, but also a concavo-convex piece of bone comprised of the greater tuberosity and part of the lesser, and extending down to the point where the humerus touches the acromion, and including even the bicipital groove as a whole with its tendon intact. (See Plate IX.)
If the force goes no further we shall have a false dislocation, for the lower part of the capsule being loose and there being no support above, the head will glide over the lower edge of the glenoid and fall into the lower part of the capsule, stretching it downward. Correspondingly, the dislocation will be at once reduced as the arm falls to the side, for it will not be pushed through a hole in the capsule and thus have an impediment to easy reduction.
.jpg)
.jpg)
PLATE IX. FRATURES OF THE TUBEROSITY AND FALSE DISLOCATION
The mechanism of fracture of the greater tuberosity and its relation to false and true dislocations.
a. The pivotal position.
6. When leverage is exerted against the acromion as a fulcrum, the biceps tendon guides the upper edge of the glenoid to enter the sulcus as a wedge, thus tending to chip off the tuberosities. This wedge is not a point but the curved edge of the fibrocartilage backed by the rim of the glenoid.
c. The inferior extremity of the fragment is therefore at the point of impaction of the acromion. The biceps tendon, tuberosity and subacromial bursa remain in their normal relations. A false dislocation of the head may then occur without rupturing the lower part of the capsule because tension is relieved by the rent in the upper portion. The lower part of the capsule, which is normally capacious, will be merely carried beneath the glenoid, as the arm descends.
d. The same lesion with the muscles depicted. A portion of the subscapularis still remains attached to the lesser tuberosity, but most of the greater tuberosity, and part of the lesser, remain in Continuity with the fragment.
e-f. Schematic drawings to illustrate the difference between a false and a true dislocation. False dislocation must necessarily be accompanied by rupture of the upper portion of the capsule, together with fracture of the greater tuberosity or rupture of the tendons. There is no structure except possibly the biceps tendon likely to interfere with its replacement, but in a case of true dislocation where the lower part of the capsule alone gives way, the sides of the capsular rent would tend to become tight around the neck of the bone, when efforts are made at reduction. In the worst cases where the two forms are combined an operation is required.
It seems as if some cases must occur in which the biceps tendon would be freed because the line of fracture might extend down the groove and the tendon would thus be separated from the greater tuberosity, and lie between the fragments. I think it usually remains in contact with both fragments if it is not evulsed from the glenoid by the same violence, in which case it retracts into the groove.
This I believe to be the mechanism in most cases of fracture of the tuberosity, whether the accompanying dislocation is recognized or not. On the other hand, both the bone and the supraspinatus attachment may hold in whole or in part, and be stretched down over the glenoid, until the lower portion of the capsule is tensed and torn and permits the head to slip through it and remain subglenoid, with the torn capsule tense on each side of the surgical neck. This will be the ordinary uncomplicated true dislocation.
Violent falls may produce a combination, first wedging off the tuberosity and then driving the head through the lower capsule.
Other variations may be:
1. Instead of the whole tuberosity being wedged off, the supraspinatus may tear away only the facet of insertion.
2. Evulsion of the supraspinatus at the blue line may occur.
3. Rupture of the supraspinatus may take place just above the palisades.
4. Very rarely a lip may be pried away from the lower edge of the glenoid instead of having the capsular attachment give way. I suspect that this is more apt to occur when the forearm is very much rotated internally and the arm is akimbo.
5. Rupture of the long head of the biceps may accompany true or false dislocation, or any of the above variations.
In general, in types 1, 2 and 3, we may expect additional tearing either toward the side of the infraspinatus or toward the side of the subscapularis, according to the degree of rotation of the humerus on the scapula at the time of the fall.
These are the very obvious lesions which may occur, but I believe the most common complication to be the " rim rents " described in Chapter V, which occur not only with dislocation, but in many cases where these structures are just able to resist dislocation, although the synovia becomes separated from the articular margin and a few inner fibers of the tendon are torn.
Another factor which may resist dislocation remains to be considered—the atmospheric pressure which holds the bursal surfaces together. In the typical false dislocation with fracture of the tuberosity, I do not believe that the relations of roof and floor of the bursa are destroyed. Until air is let into the bursa the surfaces tend to remain in contact. Many a time I have demonstrated this on the operating table. The same is true of the joint. To test in actual pounds the degree of pull required to separate these surfaces remains for some future observer. I feel confident that many pounds of direct pull would be required in the living to separate either bursa or joint to any great extent unless fluid is present. Even when the bursa is opened one cannot pull the joint surfaces apart without undue force unless the supraspinatus is torn, when they fall apart as soon as the air enters. The surface area of the bursa and that of the joint must be very nearly the same, roughly two inches in diameter, each. In X-ray tests one must remember that the cartilages do not show and that the presence of fluid permits separation.
A thorough understanding of what has been said in the preceding pages of this chapter is so important that a summary seems necessary at this point.
1. In spite of the usual histories which patients give of striking on the shoulder, the cause of dislocations or fractures is rarely, if ever, direct, but is usually a backward or downward (i.e., backward and downward in relation to the body as the patient falls) force, acting in the pivotal position, or in a subordinated pivotal position, through the humerus as a lever, with the acromion as a fulcrum, and the weight represented below by the lower portion of the capsule supported by the triceps, latissimus and teres major, and above by the resistance of the supra- and infra-spinatus, the long head of the biceps, and the atmospheric pressure in joint and bursa.
2. During a fall, unless the elbow is maintained in flexion, rotation of the humerus readily occurs; but since no lateral motion at the elbow is possible, fixation of a flexed forearm in a given position may greatly alter the direction of force applied at the shoulder, so that dislocation might occur at a point in elevation short of the pivotal position, but usually above the horizontal. For example, a lateral fall in the coronal plane when the humerus is held in internal or mid-rotation, in such a manner that external rotation is prevented (as by contraction of the pectoralis major), or a somewhat headlong fall in the sagittal plane while internal rotation of the forearm is prevented, might result in fracture or dislocation.
3. It is very unlikely that forward dislocation ever takes place unless the fall is at least somewhat headlong, i.e., one in which the elbow strikes a point anterior to the trajectory of the center of gravity.
4. In most instances subglenoid dislocation must be at first momentarily erect. The descent of the arm into the sling position, in which we usually find it, will be in internal rotation with the head of the humerus still displaced below and anterior to the glenoid, with the subscapularis relaxed and the other short rotators stretched over the glenoid. The long head of the triceps will be between the teres major below and the minor above, and the articular surface of the humerus will face backward on the origin of the long head of the triceps.
5. It seems probable that backward or subacromial dislocation never takes place from forces operating on the arm when it is being elevated, but must occur below the horizontal when the humerus is only abducted to a sufficient degree to permit the flexed forearm to be forced backward behind the body in internal rotation. Vice versa, anterior dislocation usually occurs only when the arm is above the horizontal, although theoretically, if the elbow were at the side and the humerus were rotated outward by the flexed forearm, anterior dislocation might occur from a sudden lateral fall which forced the forearm in external rotation behind the body. This would be a very unnatural way to fall, however.
If we accept the above explanation of the mechanics of dislocation, we may proceed to speculate on the reasons why fracture instead of dislocation often occurs from exactly similar falls. Age seems to be the determining factor, but this factor may be subdivided into two secondary ones, i.e., the relative tensile strength of the structures at different ages, and the relative mobility of the bones in youth and in age.
Assuming stress in the pivotal position:
In early youth the humerus ascends high under the acromion, and as the epiphyseal line is relatively the weakest point, epiphyseal separation will probably occur.
As a rule, in youth and manhood after union of the epiphyses, tendon and muscle and bone are strong relatively to the lower portion of the capsule, so that dislocation will take place. If any fracture occurs it will usually be at the greater tuberosity. Occasionally it will occur at the surgical neck.
In old age the trabecular structure about the base of the tuberosities will be weak; therefore, comminuted fracture will readily occur. If the bone holds, dislocation will usually be accompanied by rupture of the supraspinatus, for the muscles and tendons will be weak and cannot disseminate the force.
The second factor, i.e., the extent to which the head of the humerus may pass beneath the acromion, is also important in determining the seats of fracture in youth and in age.
In childhood the tip of the acromion is soft and cartilaginous, and thus the stress on the bony portion of -the acromion would be met at about the epiphyseal line, although the head of the bone passes far beneath the cartilaginous acromion.
.jpg)
FIGURE 56. EPIPHYSES OF A CHILD'S SHOULDER BONES
Outline drawing from X-ray of child with both arms elevated. By use of a dotted line the figure on the left is made to appear as an anterior view while that on the right appears as a posterior. At this age the tip of the acromion is pure cartilage and does not appear in the film. Notice that the head of the humerus passes beneath the acromion just far enough so that the bony portion of the acromion would gain a point of impact very close to the epiphyseal line. The cartilaginous tip would bend and the breaking force would occur at the epiphyseal junction.
This figure also shows that the line of epiphyseal union of the coracoid is at its base. I have never recognized a separation of this epiphysis. My work has been such that I have seen comparatively few injured children, but I think that it is quite possible that this lesion does occur, and may be detected by characteristic symptoms. It is certainly one of those conditions which we should expect on purely mechanical grounds.
In youth the tuberosity also passes far beneath the acromial edge, and this will bring the fulcrum to bear low down on the surgical neck, just above the attachment of the powerful pectoralis major. Usually dislocation will occur with or without fracture of the tuberosity. Occasionally the surgical neck will give way at the fulcrum.
In the stiff, aged joint, the tuberosity will barely pass beneath the acromion, and impact of the latter will come at the point just below the tuberosities, where the cancellated bone is weak, so that comminuted, intracapsular fracture will usually occur.
It is likely that there may be some changes in the exact lines of these comminuted fractures according to the degree of rotation which the humerus attains at the time of fracture. That is, the acromion will be applied at quite different points on the tuberosity in external and in internal rotation.
Other factors may be important also. For instance, the rapidity of the application of force; the degrees of contraction of the various muscles; congenital or habitual variations in the structure or position of the bones and of other tissues; the weight of the body; many minor circumstances or unusual combinations of any of the above factors. However, the point I wish to make is that the pivotal position is to the human arm in its varied activities as his earth is to the fox. The elusive arm must be driven to its pivotal position to be caught, or tricked by preventing rotation on the way. With continued effort we may always dig the fox out, and with continued backward force we may always break or dislocate the head of the humerus,, although the human arm is as clever in evasive rotation as the fox is in doubling.
There are many other points on which a consideration of the "Pivotal Paradox" is enlightening and which are worthy of study, for a thorough understanding of the mechanics of dislocations must be of help in their diagnosis and treatment. However, it will require many studies by many people before practical experience will cease to be our guide. Whether the deductions I have made above prove to be right or wrong, the following practical facts support them and are confirmed by all writers and by each surgeon in his own experience.
The causes of anterior dislocations are usually headlong or lateral falls with the arms thrust forward to fend off the ground.
The same kinds of falls may also produce the following lesions of the upper end of the humerus:
(1) Separation of the humeral epiphysis.
(2) Fracture of the surgical neck.
(3) Fracture of the tuberosities.
(4) Fracture of the anatomic neck.
(5) Comminuted fractures in which the typical form consists of four fragments; i.e., the two tuberosities, the anatomic head, and the shaft. (See Fig. 60.)
Any of these forms may be complicated by concomitant dislocation of the articular head, whether or not it remains attached to the shaft.
The fractures will be discussed in the next chapter and dislocations in the remainder of this one. However, the two subjects are inseparable and one should realize that both fracture and dislocation occur in many cases which are classed as either lesion. I am inclined to think that a combination is the rule, especially in cases of fracture of the tuberosities, and that many supposedly simple fractures are accompanied by false dislocation of the head which immediately becomes spontaneously reduced. Previous dislocation is evident in cases of complete separation at the anatomic neck in which the head remains displaced, but unless the latter is completely separated, it will be dragged back by the tuberosities, which are rarely dislocated because they are sucked back by the bursa and almost invariably remain attached to the short rotators. In other words, these tendons may rupture without the occurrence of any bone lesion, but if one does occur, the tendons remain attached to the fragment. Only small crumbs of the tuberosities ever become really free even in the most comminuted fractures.
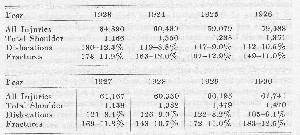
The number of shoulder injuries compared to the total number of industrial accidents reported in Massachusetts during eight years is shown in tabular form. This table is not perfectly accurate, so far as the figures on dislocations and fractures are concerned, because it was not arranged for the particular purpose for which I am using it. For instance, all fractures of the clavicle and all fractures of the humerus are included because no distinctions had been made as to the part of the bone injured. It is probable, therefore, that the number of dislocations is fairly exact, but that the number of fractures of the upper end of the humerus is considerably less than the figure given, and probably in every year less than the number of dislocations. Probably many of the cases which were classed as fractures also had dislocations and vice versa. Although there is a striking tendency toward uniformity of the numbers through the different years, the proportion of dislocations to fractures varies somewhat for the above reasons. It is fairly safe to say, however, that about one-fifth of all shoulder injuries occurring in industry are fractures or dislocations of the upper end of the humerus. It is likely that if we could get similar statistics from the population not engaged in industry, fractures would be more common than dislocations, because fractures in this region usually occur in elderly people. Unfortunately, there can as yet be no statistics to determine how often the supraspinatus is injured as a complication of these so-called major (?) injuries, nor what proportion it forms of the other injuries which are unclassified. I believe that it costs our community more than all the other lesions together, not only because it is so common as the major lesion in fractures and dislocations, but because there are many unrecognized minor cases.
The shoulder is the most frequently dislocated joint in the body. This fact is quite properly generally ascribed to its relative instability. Dislocation of the humerus occurred 108 times in 528 cases of dislocation reported by Eliason, and it has been stated by various authors that forty to sixty per cent of all dislocations are of the shoulder. Many shoulders are probably dislocated and immediately reduced by the patient or his companions as they lift him after a fall, without knowledge that dislocation has occurred.
Dislocations of the head of the humerus have been classified in several ways, although for practical purposes only two classes are of importance, i.e., the forward or subcoracoid, and the backward or subacromial forms. As the latter are rare, "dislocation of the shoulder" usually refers to the former.
.jpg)
The first four varieties in the table are essentially the same. If the tear of the capsule and stretching of the muscle bellies away from their beds-are extensive, the dislocated head can be moved easily from a subglenoid to a subcoracoid or to even a subclavicular position. As has been shown, the erect subglenoid position probably occurs in every case momentarily, as the patient falls with the upraised arm, although depression and internal rotation at once ensue from muscular contraction, causing the arm to assume the position at the side in which we usually find it. Very rarely does the erect phase last long enough to be classified!
Subspinous is merely an extreme degree of subacromial dislocation. It occurs when the infraspinatus has been badly torn from its bed so that a large space under the spine of the scapula accommodates the displaced head. Upward dislocation implies an accompanying fracture of the acromion and is nothing more than a curiosity in extremely severe accidents. I have never seen it.
DIAGNOSIS OF ANTERIOR DISLOCATION
In simple subcoracoid dislocation of the humerus, the well-known signs are as follows:
- History of a trauma to the shoulder in which something was felt to give way and a severe, acute, nauseating pain was experienced.
- Active and passive movements are limited and painful.
- The forearm is held flexed and internally rotated.
- The elbow is away from the side and cannot be completely adducted, thus causing the long axis of the shaft to incline upward and inward.
- Patient stands inclined to the affected side so as to bring the axis of the humerus to a vertical position.
- Measuring from the acromion to external epicondyle, the upper arm appears lengthened.
- The anterior axillary fold (on the affected side) is lower.
- The shoulder is flattened.
- The acromial process is prominent.
- The head is palpable under the coracoid.
- A soft crepitus can be elicited while manipulating the shoulder.
In other words, the facts to be learned from the history, inspection, palpation, motions and mensuration, plus the aid of the X-ray, will usually make the diagnosis beyond doubt. In fact, the diagnosis is generally so obvious that we must be on our guard not to overlook concomitant injuries and complications. While examining the patient one should take especial note of the circulation of the arm, and of the sensitivity of the skin over the arm and shoulder. The power of the deltoid, rhomboids, clavicular part of the pectoralis major, supraspinatus and infraspinatus, etc., should be carefully noted with a view to detecting paralysis. When the case is typical, the eleven signs are exceedingly plain, but this does not mean that when they are absent there is no dislocation.
It is very important for the reader to understand that all of the above signs, except the first and the last, fail when the articular head has been replaced on the tuberosity, which has itself been displaced into the glenoid. At this point the reader should refer to the history of Case 71, page 288, and study the accompanying diagrams. Our mistakes in diagnosis will occur in these cases where the head of the humerus can hardly be said to be out of place, but is certainly not in place, for the short rotators with the evulsed facets lie between it and the glenoid. (Fig. 58 and Case 115, p. 389.)
The second symptom was absent in Case 115 because the nerves were paralyzed or so retracted as not to be influenced when the arm was moved. The replacement of the head to nearly its normal position had completely removed the third to tenth symptoms and even the eleventh symptom, in this particular case, was absent or very difficult to detect.
Of course, such cases of pseudo-reduction are not common, but they occur now and then, so that we must never fail to bear in mind that cases of dislocation which are not quite satisfactory may become extremely unsatisfactory, if the supraspinatus or other short rotators are torn, or have dragged the facets toward the glenoid.
Treatment. The main therapeutic principles are: reduction, fixation and gradual return to function.
Reduction in most cases can be obtained by the Kocher or by the Astley Cooper traction methods. These procedures are too well known to describe in this text. The Kocher method is most generally used because much less force needs to be exerted, and hence less trauma should occur during the reduction. However, as Kocher himself said in his original article, it does not always work and it is sometimes necessary to use the Astley Cooper method.
Much has been said concerning the optimum position in which to maintain reduction. This would seem to suggest that the ideal position had not been found. Some modern authors, notably Stevens, are of the opinion that the arm should be put up in abduction and external rotation.
A simple way of obtaining abduction and external rotation is to put the patient in recumbency, and fasten the hand to the head of the bed. A suitable ambulatory splint can be used, or both methods in conjunction. A splint maintaining abduction and external rotation is cumbersome, and attracts a great deal of attention. The ordinary airplane splint abducts, but internally rotates the arm. Abduction and external rotation put the patient in the position of a traffic officer stopping a line of cars. The writer does not advocate this abduction treatment, and prefers not to fix the arm at all.
The advocates for maintaining the arm in the sling position after reduction, contend that the torn capsule heals better because it is relaxed. This seems reasonable, unless the rent is longitudinal, in which case its edges would be approximated better in abduction. It has never been determined positively whether rents in the capsule are usually longitudinal or transverse. Some writers claim that the capsule is torn from the forward edge of the glenoid, and my opinion is that this is the usual condition, for this only means the tearing of the pillars which form the opening of the bursa subscapularis. More observations of cases where death has occurred from the same accident as that which dislocated the limb are much needed. If we knew in general how the capsule is usually torn, the answer to the question of whether to maintain adduction or abduction would be much more plain.
The writer believes that at present there is too great a tendency to confine the arm after reduction. It would seem more logical to let the patient use his arm a little—even to urge him to do so, in order that debris and blood clot may work out of the joint capsule into the areolar tissue, where they would be readily absorbed. If the capsule were emptied of the blood clot, it would seem that it would be more likely to have its edges fuse together again without leaving any distortion or undue irregularity. On the other hand, I believe that motion should not be forced for fear of tearing edges which are beginning to unite. For those who think this policy too radical, it would be safer to treat most cases in the sling position than in the abducted one, unless the surgeon were very well versed in the study of the shoulder joint. I think stooping exercises should be begun at once and continued daily in any case. We should use fixation only for comfort, and this means very little, for one may be sure that if there is severe pain after reduction some complication exists.
Prognosis. It would seem an easy thing to make a prognosis in cases of dislocation, but as will be seen shortly, complications are frequent, often unrecognized, and greatly modify the period of disability. A fair prognosis in uncomplicated cases would seem to be a return to normal function in from four to eight weeks. However, complications are, I am sure, more frequent than is generally realized.
.jpg)
FIGURE 57
X-rays of the case alluded to in the text in which the articular head had become displaced beneath the deltoid and was excised through a sabre-cut incision. This patient recovered with a useful arm, and was able to play excellent golf for many years afterwards. Undoubtedly fracture and dislocation occurred at the same time, and the head was left behind in the erect phase of dislocation, when the arm came to the side. The articular surface remained in nearly the position which it occupies in normal elevation. It seems possible that if this fact is recognized in similar cases, reduction might be accomplished by again placing the shaft in elevation, opposing the raw surface of the articular head to that of the tuberosity, and holding them together while the arm is brought to the side in the coronal plane.
Figure a, before operation.
Figure b, a few months after operation. The acromion, which had been sawed across for the sabre-cut incision, has been wired about two steel pegs.
Figure c, taken nineteen years later, when the patient was eighty. There had been no trouble from the wire or pegs in the intervening years. At this time motion in the joint still persisted, but "was very limited in degree. However, it was sufficient to permit a slight amount of abduction and rotation, which permitted him to use his arm freely for ordinary purposes. Although this operation was successful in restoring a fair degree of usefulness, if I were obliged to operate again for such a condition I should not remove the articular head, and would endeavor to reconstruct a normal joint, perhaps employing Dr. Nicola's suggestion of anchoring the articular head by means of the biceps tendon. Before incising, I should hyperelevate the arm in internal rotation in order to appose the fractured surfaces.
Gubler, in a study of insurance records of 252 workmen's compensation cases, states that recovery occurred in 94.1% of the cases after an average of thirty-eight days of treatment. Another investigator, Kuttner, reports a far different experience. He was able to trace fifty-four uncomplicated cases from among 168 treated during the previous five years. Only seven (13%) had regained full use of the limb without loss of strength or motion. In fourteen (26%) the range of motion was complete, but the strength was reduced one-half or more. The remaining thirty-two (61%) had some loss of motion, which in twenty-six amounted to inability to raise the elbow laterally above the level of the shoulder. He states that all of these cases were uncomplicated (which we doubt), and had been treated in the hospital by immobilization for a week, followed by massage and mechanotherapy for two to three months. Goebel reports similar unfavorable results on twenty-four patients. Twelve had full function, but subjective complaints. Twelve had limitation of motion. Lexer reports forty cases; ten with complete restoration, fifteen with some limitation, fifteen with pain and loss of strength.
These reports are self-explanatory, and coincide with my observation of results obtained in general hospitals. The conclusion is that most of these patients received other injuries at the time of the accident or during treatment. I believe that uncomplicated cases tend to recover in about four weeks, unless interfered with by injudicious treatment, such as prolonged fixation.
Complications. Injuries to other structures about the joint are common and students should be most thoroughly warned of this fact. It is not so much that these complicating lesions are difficult to detect at the time of the first treatment, but that they are not suspected. It is a fact that these complicating lesions do often exist and do maintain disability and pain long after the joint itself has returned to normal, yet there is no organized effort of our profession to correct this condition. Industrial cases may be labelled malingerers, psychoneurotics, hysterics, or cases of traumatic neuroses, because of this prolonged disability with few detected physical signs. The five common complications of dislocation are the following:
- Fracture of tuberosities.
- Avulsion of the facets, or rupture of the tendons.
- Fracture of the glenoid rim of the scapula.
- Injury to the brachial plexus.
- Rupture of the axillary artery or of other vessels.
Fracture of the greater tuberosity has hitherto been thought to be by far the most common injury accompanying dislocation. Graessner found the greater tuberosity broken twenty-four times in forty-eight dislocations, but in many of them the fragment was only a small scale of bone, indicating an avulsion of the tendon. Delbet found it in twenty-two out of one hundred and ten cases. Dollinger in five out of thirty-nine. Goebel twenty in forty-three cases. Schlaepfer found it eight times in one hundred and twenty cases, or 7.4%. Gubler reports it in eighteen out of two hundred and fifty-two cases, or 7.1%. Gubler also reports ten cases of other bone injury, and ten of nerve injury in his series. In my opinion, many of the cases where only a small facet is torn away should be classed with supraspinatus injuries rather than with fractures of the tuberosity, because they result in free communication between the joint and the bursa.
The bone injuries are generally easy to diagnose if looked for. The typical signs of fracture, especially ecchymosis down the arm along the biceps, are usually present and the X-ray is of great assistance. The real difficulty is too great a tendency to treat the major abnormality, the dislocation, and to overlook very important, but less obvious, injuries. Sometimes failure to recognize complications is due to careless X-ray examination, but more often to the inexperience of the doctor who first treats the patient. Rupture or avulsion of tendons attached to the tuberosities should be suspected when the films are negative.
The injuries to nerves and arteries will be considered in Chapter XI.
REFERENCES OF AUTHORITIES TO THE ROLE OF THE SUPEASPINATUS
IN DISLOCATION
Little is to be found in the literature to confirm my beliefs or to explain why the short rotators come to be so frequently injured. Only a few writers have realized the frequency of such injuries, and I do not think that any" of them have appreciated the significance of the fact that the bursa and joint are thus put into communication.
Stimson says that the supraspinatus is sometimes, probably often, torn from its attachment to the humerus, and the same is true in less degree of the infraspinatus, and occasionally even of the teres minor. He states also that avulsion of the tuberosities may take the place of laceration of the tendons. Preston says that injury to the capsule is not infrequently accompanied by injury to the tendons which overlie and reinforce it, and when the violence producing the luxation is great, there may be a destruction of tendon continuity.
Stevens gives an excellent description of shoulder dislocation with especial reference to the short rotators. According to him, an anterior dislocation is an impossibility without putting a strain upon the tendons of the supraspinatus, infraspinatus and teres minor. With the humeral head in subcoracoid dislocation, the distance from origin to insertion of the supraspinatus is greatly increased, and in addition the tendon is angled over the rim of the empty glenoid. Similarly the posterior rotators are pulled over the posterior rim of the glenoid, and are almost always injured. "We may," he says, "assume that in every case of dislocation of the humerus, and especially in anterior dislocation, there is an injury to the tendon of the supraspinatus, and that often it is ruptured."
Very few other authors even allude to this tendon.
The following cases as well as the above quotations from the literature support the assertion that the facet of the supraspinatus may be torn off in dislocation.
CASE REPORTS
No. 12. Mr. A. F. K. Age 45. Massachusetts General Hospital No. 174082 W. S., Jan. 23, 1911.
A subcoracoid dislocation of four months' duration. Open reduction of dislocation. Supraspinatus was found retracted with facet of insertion. Heavy silk sutures to unite it with tuberosity. Feb. 24; 1912: An excellent functional result, but scar is ugly.
No. 22. Mr. J. H. D. Age 69. Massachusetts General Hospital No. 182238, April 22, 1912.
Five weeks ago fell, injuring right shoulder. Reduced by M.D. Went back to work. One week ago dislocated it again when drunk. I made an unsuccessful attempt at reduction in the Accident Room, and then carried the patient under ether to the operating room, and through the usual incision for the bursa I opened directly into the joint. A defect corresponding to the facet of the supraspinatus was found, the supraspinatus being retracted under the acromion. There was no piece of loose bone corresponding to the defect, although the whole joint was carefully searched. It must therefore be assumed that the loose piece had been absorbed. The dislocation was reduced, supraspinatus reinforced with silk and the wound closed. Two years later he wrote me: " I can do quite a lot with it, only when I reach overhead it gives way and causes some pain."
No. 71. Mrs. E. C. Age 68. On June 10, 1921, fell downstairs, broke left wrist and dislocated left shoulder. Ether was given by the local doctor, and he supposed he had reduced the dislocation. She consulted me on August 9, 1921, and after taking X-rays, I reported to the physician who had sent her to me that I thought that the shoulder joint had been reduced. The accompanying X-ray seemed to me to show that the bone was in place. I know now that this appearance is deceptive. In such cases as this, the tuberosity has been retracted into the glenoid and the head of the humerus rides on it. Therefore, there is not very much change of contour in the position of the shoulder, because the total amount of bony substance between the tip of the shoulder and the glenoid is the same, although the position of the tuberosity is reversed and lies in the glenoid. The following is an account of the operation which I did on April 5, 1922, nearly a year after the injury.
Sabre-cut incision. Prominent anterior mass proved to be head of humerus minus the tuberosity. The tuberosity had been retracted by the posterior short rotators and lay partly in the glenoid cavity and partly overlapping its posterior margin. The biceps tendon was displaced so as to lie between the head of the bone and the glenoid. It was excised. The retracted tuberosity was also excised. The synovial and tendinous capsule of the joint was completely gone, except at the anterior edge, namely, the portion formed by the subscapularis tendon. A good, practical result was obtained, i.e., a movable, painless, weak shoulder, lacking power in abduction, but more useful than a painful joint.
It is my belief that in most of these cases of dislocation where the X-ray shows a portion of the tuberosity to be absent, careful pictures will show its presence in the glenoid or just below the glenoid. The capsule forms a pouch below the glenoid and this pouch catches the smaller fragments if they have become loose. The cases are deceptive because a reasonable amount of motion may be found within the first few weeks and the position of the head is so nearly normal that it is not realized that the head does not actually touch the glenoid.
.jpg)
FIGURE 58. THE USUAL CAUSE OF FAILURE TO REDUCE A DISLOCATION
Mrs. E. C.— X-ray (a) before the local doctor attempted reduction. The fragments of tuberosities may be seen external to the lower edge of the glenoid. The head of the bone is displaced far beneath the coracoid process; the form of dislocation might be classified as subclavicular. It is probable that in this case there was both a true and a false dislocation. After reduction (b) the tuberosities seem to be absent, though indications of their fragments are shown near the lower edge of the glenoid. I have operated upon a number of other similar cases (e.g., Nos. 5 and 92), so that I have formed the opinion that when the X-ray after reduction shows the absence of the tuberosity, radical operation is indicated, even if the X-ray does not demonstrate the fragments. It is my belief that this form of displacement accounts for the great majority of instances, which the authors quoted in this chapter speak of, as unsatisfactory results.
Case 115, to be reported later, was also an illustration of this condition. Two of the most alert industrial surgeons whom I know were fooled by the superficial appearance in this case, and I, myself, did not recognize it on my first visit. Even Stevens, whom I regard as having been particularly well informed about conditions in the shoulder, shows in his illustration, "Fig. 4," what I believe to be a case of this kind. He speaks of the fragments as having disappeared behind the head of the humerus. In cases showing X-rays similar to this, I would recommend exploration through the routine incision of the bursa. If it is obvious that the fragment has retracted into the glenoid, I recommend enlarging the incision to a "sabre-cut," and making an attempt to suture the structures in their normal position.
Before leaving the subject of anterior dislocation, I should like to italicize the following paragraph:
I believe that after the reduction of every case of dislocation of the humerus, the patient should be allowed to recover from the anaesthetic and be urged to move his arm freely, before any bandaging is applied. All motions may be safely performed except abduction in external rotation, and even this may be done with due care and using extension at the same time. If we find paralysis of any of the muscles, areas of skin anaesthesia, undue axillary swelling, gritting sensation in the joint, or a tendency for the joint to slip out of place, the patient should be at once hospitalized and consultation obtained.
(The author here advises the reader to study the next chapter on fractures and then to return to the remainder of this chapter, which discusses some of the more unusual forms of dislocation.)
.jpg)
FIGURE 58
(c) Explanation. Erect dislocation, as usual, preceded the subcoracoid position. The fragments of tuberosity, still held together by the musculo-tendinous cuff, slipped down on the glenoid, while the head was dislocated below and the arm fell to the side. Reduction was attempted and seemed successful, but the head of the humerus merely became superimposed on the fragments so that it seemed that the dislocation had been reduced, and the contour of the swollen shoulder became nearly normal. The biceps tendon was carried with the fragments on to the glenoid. In Case 115 there was scarcely any fracture except at the facets of insertion; the whole musculo-tendinous cuff had dropped back on the glenoid. In most cases the retracted tuberosities are held on the glenoid by the short rotators, as this man holds his hat on the further side of the tree. The biceps tendon may (Case 115) or may not (Case 71) be torn in such cases.
Subacromial dislocation is rare. I can only recall one case in private practice. This was in a young man who was a personal friend. It is twenty years since I reduced his dislocation, immediately after the accident, and the shoulder has given him no trouble since. Probably most of these subacromial or subspinous cases run as smooth a course, but occasionally, as in the following instance, one proves to need operation.
No. 33. Mrs. C. B. Age 38. Massachusetts General Hospital No. 184814 W. S., Sept. 7, 1912.
A case of recurrent subspinous dislocation which had remained unreduced for three months. "Sabre-cut" incision, the joint carefully inspected and cleaned of old granulations and detritus. None of the short rotators had been ruptured. Dislocation reduced and acromion wired in place. April 17, 1914, she writes, "I am thankful to say my shoulder is all right. It does not seem to be as strong as the other one, otherwise it is fine."
This is the type of case in which the "sabre-cut" incision is particularly applicable, in fact, it is almost indispensable if one wishes to obtain a satisfactory cleaning out of the glenoid. In all these operations for old dislocations I have found the glenoid to be filled with old granulations and detritus. Satisfactory reduction could not have been done without thorough cleaning of the cartilaginous surface.
The second case is an illustration of what I believe to be the usual mechanism of subacromial dislocation. She gave the history that seven years previously the first dislocation had occurred, during a convulsion while she was in labor. Six months later she dislocated it again while " closing a door behind her." The last time it was dislocated by "turning quickly around in her chair."
In the case first mentioned, the young man sustained his injury while being thrown from a sitting posture on a toboggan which had struck a rock. He was thrown in the air—presumably still holding the railing of the toboggan. This might produce the same effect of internally rotating the arm, as in closing a door behind the back.
OLD DISLOCATIONS
Speed considers a dislocation as old and irreducible after three months. The obstacles to reduction are the same as for a simple dislocation plus such secondary changes as:
- Cicatricial contraction from healing scars in the capsule and adhesions to surrounding structures.
- Displaced bone fragments, osteophytic outgrowths, callus, etc.
- Muscles shortened and atrophied.
- Synovial space obliterated
One can readily understand the difficulty of reducing an old dislocation if he will study the specimens to be seen in anatomic museums. The remarkable attempts of nature to derive some utility from a dislocated shoulder joint make reduction most difficult. At the point where the humeral head lies against the scapula, a tremendous bony proliferation takes place, and inevitably ankylosis or pseudoarthrosis results. The glenoid becomes atrophied and filled with fibrous tissue.
The varying combinations of pain, deformity, and limitation of motion which these patients present have incited surgeons to attempt relief. Every surgeon of large experience htts probably made a few attempts to help such patients, but before long finds that they form a class of cases in which he can be generous to his younger colleagues, who also in time learn by experience. As a matter of fact, these are serious cases and demand expert care, although this is not attainable at present, for there are no such experts, so far as I am aware.
There are five general lines of treatment from which we may choose.
(1) To leave nature to do the best she can.
(2) To attempt bloodless reduction under an anaesthetic.
(3) To attempt open reduction.
(4) To resect the head of the humerus.
(5) To perform arthrodesis.
Andrews concluded that an attempt at reduction by manipulation is extremely dangerous. In his words, "The bloodless method has a gory trail of accidents." He finds fifty cases of hemorrhage, mostly fatal, up to 1905. An interesting one was reported by J. C. Warren, in whose case a large aneurysmal tumor arose after attempts at reduction. The subclavian was tied and recovery ensued.
If a new joint can be produced at all, it should be possible to do it by the "sabre-cut" incision, for all the structures of the joint are readily visible and accessible. I have encountered two chief difficulties. One has been the fusion of the retracted tendons and tuberosities with the glenoid alluded to in Case No. 71. If many months have passed, there is little left of the cartilaginous surface of the glenoid when the debris has been removed from it. However, this is not the chief obstacle—the real one being the absence of any synovial membrane to prevent adhesions of the cartilaginous head in its new bed. If the cartilaginous head is not too badly destroyed and seems likely to function, I should advise completing the attempt to make a new joint, but if the head has been eroded and there is no synovia left to surround it, adhesions will surely take place, and almost no motion will be secured. An irritable, painful joint with only a few degrees of mobility will result. In such a case, I think that one should deliberately perform excision or arthrodesis. The method of arthroplasty recently suggested by Dr. Laurence Jones of Kansas City offers a most hopeful solution of this problem.
RECURRENT OR HABITUAL DISLOCATION OF THE SHOULDER JOINT
Recurrent dislocation is not a common lesion, but it has interested a large number of investigators. Speed says that this lesion is peculiar to athletes and epileptics. This is more than a witticism, but not entirely true. Almost every author has put forward a somewhat different theory as to the cause of recurrent dislocation, and Speed has gathered together the most important ones. They are:
-
Defect in the head of the humerus acquired at first dislocation, or perhaps congenital.
-
Defect in the glenoid—acquired fracture of the edge, or congenital shallowness.
-
Rupture of the insertions of the external rotators of the head of the humerus.
-
Avulsion of tuberosities with or without rupture of the rotators.
-
Detachment of capsule from anterior lip of glenoid.
-
Enlarged joint from relaxed capsule following tears which have been given insufficient time for strong cicatrization, or repeated stretching without tears.
A seventh theory may be added. Since the shoulder joint is not a real joint, and is dependent for its integrity on a very complicated neuro-muscular cooperation, the essential feature in some of these interesting cases may be a failure of this cooperation. Reference to Plate I will show how easily incoordinated pulls from two opposing muscles might result in instability of the head on its fulcrum. Rupture or stretching of the tendon of the latissimus might thus make the joint unstable in the pivotal position. Certainly from an X-ray point of view the bony structures in most of these cases are normal.
The slight support furnished the joint by the bony structures has been considered, and it would seem more reasonable to suspect a defect in the major supporting structures, the muscles and their tendons, than in the bony structure. The importance of the supra-spinatus and of the other short rotators has been emphasized, and it has been noted with what frequency their continuity is broken in ordinary dislocations. More authors have found occasion to mention lesions of the short rotators and tuberosities in recurrent dislocations than in simple dislocations, because the majority of the former cases are treated surgically, so that more opportunity is afforded for observation.
Considerable evidence is given in favor of each of the causes listed by Speed and probably any one of them could well account for a recurrent dislocation. Hildebrand found two cases of fracture of the anterior rim of the glenoid with laceration of the capsule, in which he obtained good results by reshaping and deepening the glenoid. In an X-ray study of twenty-one cases in Hildebrand's clinic in Berlin, Pilz found definite bony defects in the humeral head in fifteen, de Fourmestraux found a deformity of the head in four out of eighty cases. Henderson reported no bone injury found by X-ray in many cases. We have seen several cases in which no abnormality could be found with careful X-ray examination.
According to Stevens recurrent dislocations at the shoulder joint are always due to more or less tearing of the supraspinatus, infraspinatus, teres minor, and more rarely of the subscapularis, and their subsequent repair by scar tissue in a position of stretch. No definite cases to prove this were given.
Thomas concludes that habitual dislocation is due to a traumatic, cicatricial, anterior, hernial pouch of the capsule. The most constant lesion which he found was a tear in the anterior and lower part of the capsule. In an experimental luxation of the shoulder on a cadaver, he placed the head in complete subcoracoid dislocation, and found the supraspinatus, infraspinatus and teres minor not torn or greatly stretched. However, any assumption that such lesions do not occur in the living is unwarranted, for the conditions are so different. In such experiments lax atonic tissues replace the living contractile muscles, and the force is gradually and gently applied as compared to the sudden smashing force acting in the living. A force suddenly applied against active muscles would have much greater rupturing power than a much greater force evenly applied against dead muscles.
One of the earliest mentions of the role of the supraspinatus was by Duchenne, who wrote: "Recurrent dislocation cannot occur with a normal supraspinatus." Yet I do not entirely agree with this great authority, for in none of my cases of habitual dislocation have I demonstrated such a rupture, and in two I actually did demonstrate that there was no rupture. Furthermore, I have never seen habitual dislocation complicate a case of ruptured supraspinatus.
Speed states that the head of the humerus twists out of the glenoid through the inferior portion of the capsule, and he believes that to permit this dislocation there must be a great strain on the supraspinatus tendon, or even a tear in it.
It is in the treatment of these recurrent cases that the greatest variations of opinion are to be found. Almost every author has contributed a different technique. The surprising thing is that so many varied methods should produce such uniformly excellent results as are claimed for them, yet the number of methods suggests that none is highly successful. The essential points of some of these methods of treatment will be briefly given with their results, when obtainable. Many of the reports are based upon too few cases followed for too brief a period. It is noticeable that few authors have reported later series in a second paper, and this suggests that the late results and greater experience have not supported them in their early statements.
Treatment.
Two general principles of treatment have been applied to habitual dislocation. They are:
- Prevention—control primary dislocation, and allow healing of capsule.
- Reconstruction.
A. Suspending head of humerus from above.
B. Support from below.
1. Reefing.
2. Bone operation on glenoid.
C. Combinations of above.
D. Use of the long head of the biceps as a round ligament.
A shearing-off of the attachment of the capsule to the fibrocartilage of the glenoid is described by Bankart as the cause of recurrent dislocation. The defect is permanent and his operation aims to repair the rent. His incision runs from above the clavicle downward and outward over the coracoid for about five inches. The deltoid and pectoralis major are separated, not cut, and the coracoid divided and driven downward with the muscles attached. The subscapularis tendon is divided and the capsule sutured to the glenoidal labium. The subscapularis and coracoid are sutured in place. Four weeks of rest is followed by active and passive motion. Four successful cases are reported.
Carrell, who gives the above classification of treatment, uses an ingenious combination of A. and B. An anterior incision exposes the long head of the biceps. The tendon is sectioned at its lowest level, and reflected from its sheath to where it emerges from the capsule. The distal end of the muscle is attached to the short head. To the free tendon is attached a piece of fascia about six inches long. A posterior incision running down four inches from the acromion separates the deltoid and exposes the teres minor. The fascia is passed under the neck, weaving in and out of the capsule. It emerges just above the teres minor and is passed through a drill hole in the acromion. The arm is immobilized at the side and motion begun in three weeks. Good results are reported in four cases. One wonders whether the posterior incision can be made without injury to the circumflex nerve. Recently Fowler has suggested a modification of this suspension operation. The biceps tendon is not interfered with, but a strip of fascia lata is passed through the capsule below the neck and anchored, both on the acromion and on the coracoid.
A bone transplant was placed by Eden under the raised periosteum of the neck of the scapula so that one-half to one centimeter stuck out in front of the joint. He also reefed the capsule and kept the arm abducted for three weeks.
Henderson's tenosuspension operation has been popular in America, but as seen by the discussion following Fowler's paper, it cannot be a thoroughly satisfactory procedure. Keller uses a crucial plication of the capsule through a posterior incision. Loeffler places a band of fascia from the greater tuberosity of the humerus to the acromion. Mandl used Finsterer's operation with success. The head of the humerus is held back by a band on the anterior surface of the joint, taking the place of the normal joint capsule. The band is composed of "part of the coraco-brachialis and part of the biceps." Oudard divides the subscapularis and overlaps it so as to shorten it about three centimeters. The tip of the coracoid is cut and a bone graft three to four centimeters long is inserted between base and tip. The coracoid may be slit and one-half slid down so as to lengthen the coracoid three centimeters. Nine cases were treated successfully. Six additional cases are reported. Perkins devised an operation in 1906 for suture of the torn capsule and reports good results. A restraining ligament was made by Plummer and Potts using a fascial strip from the greater tuberosity to the acromion. They report two cases with good results. Nine cases of recurring dislocation were treated in a year by Riviere, who pleated the capsule by placing interrupted sutures through the subscapu-laris. Landes uses a fascia lata cord or several silk sutures and suspends the head of the humerus by passing this cord through a drill hole and slinging it over the clavicle just lateral to the coracoid. Selig, who considers atrophy or rupture of the external rotators the main cause of habitual dislocation, makes an incision through the supraspinatus fossa, separates the trapezius fibers, and shortens the supraspinatus tendon by plication.
It is Sever's belief that the subscapularis and supraspinatus prevent dislocation when the arm is elevated by opposing the pectoralis major, which adducts and draws the humerus forward, and pulls the upper part of the humerus inward and downward. He says that in all operations for recurrence, the good comes from cutting the pectoralis major and shortening the subscapularis. No results are stated. He notes that repair of the infraspinatus and supraspinatus can also be done at the same time. Other authors, notably Allis, have also held similar views.
The operation advocated by Speed is done through an incision just below the coracoid and extending down four inches. The pectoralis major is divided one and one-half inches from its insertion into the humerus, and the axillary structures put aside. The edge of the glenoid is next palpated, after which, a drill hole one inch deep is made diagonally into the neck of the scapula. A bone transplant from the tibia is driven in with three-fourths inch projecting. This is supposed to prevent the head of the humerus from slipping out forward into anterior dislocation, at the same time not interfering with the normal range of motion.
A heavy silk ligature reenforces the anterior part of the capsule in the operation of Spitzy. A curved incision exposes the deltoid insertion, which is cut and retracted. A heavy silk ligature is passed around the surgical neck and tied in front. The ends are left long so that they can pass upward anterior to the capsule, and be tied over the coracoid. The capsule is then folded over the ligature and sewed, thus shortening the capsule. The deltoid is re-attached, and after a rest period of four weeks exercise is begun.
Thomas was an exponent of the capsule pleating operation. He used a posterior axillary incision, and took a reef in the capsule. He claimed exceedingly good results, as do the others. He performed capsulorrhaphy on eighteen epileptics suffering from recurrent dislocation. Twelve cases were successful, for a time at least. A capsule pleat and fascial transplant across the front of the joint is performed by Valtancoli, who reports eighty-six per cent cures.
It would seem that a patient stands some chance of cure by any of these methods. Therefore, it would be to the patient's advantage to choose the simplest, since his chances of recovery are as good as if he had the most complicated one. It is interesting to speculate why such a diversity of treatments should produce so uniform a result. It may be explained by the temporary or permanent limitation of joint function consequent to the operation. Some of the above procedures have as an object the limitation of motion, and all of them probably do limit motion. The trauma of the instrumentation, the bleeding and exudate, and the placing of sutures result in the formation of scar tissue. In addition the arm is immobilized for a time. Fixation and a sensitive scar produce pain on motion, and a certain mental impression which results in a patient's using his arm in a very gingerly way for a long time. Actual limitation or voluntary limitation are important reasons why the arm is not soon again moved into extreme elevation. It is highly probable that the late results of all these methods would not be entirely satisfactory.
Some authors have advocated and devised external apparatus to check abduction within a safe limit. These hobbles are a nuisance and offer no cure, but do prevent dislocation. The lesion is annoying and causes so much disability that many of these cases beg for operation. The treatment should be suited to the type of lesion and to the habits of the individual patient. Bony defects should be repaired or modified by plastic methods. Nicola's operation seems to be applicable, whatever the cause.
The writer has on two occasions done negative exploratory operations for this condition by opening the bursa but without entering the joint. The following case may be of interest to those who believe that deformities of the head of the bone may be the cause of recurrent dislocation, for in this patient a thorough exploration was done.
Case No. 24. Mr. K. N. Age 26. Massachusetts General Hospital No. 182833 E. S., May 22, 1912.
A large, powerful young man. First injury six months before while wrestling. Repeated dislocations after slight muscular efforts since then. "Sabre-cut" incision, supraspinatus divided and joint explored. The capsule was found to be torn, especially the portions at the lower and inner edge of the glenoid. A sort of hernia of the synovial membrane existed, which evidently made a pouch for the head when dislocated. A plastic repair was done on this part of the capsule. Part of the articular surface was missing, as if it had been broken off and absorbed. The patient was seen by me about a year after the operation, and at that time had a perfect result. I have not been able to trace him since.
This particular condition of axillary tearing of the capsule has been described by Thomas of Philadelphia, and considered by him to be the most common lesion in shoulder injuries. I have little doubt that it is a factor common to all recurrent dislocations. One cannot imagine dislocations occurring without a tear of the capsule of the joint. In all these cases the pillars of capsule which bound the opening of the bursa subscapularis must be more or less torn to enable the head of the humerus to lie in the subcoracoid position.
I have seen numerous cases of habitual dislocation, but owing to my lack of faith in any particular technique I have done few operations. I have been content to teach the patient about the mechanism of dislocation and explain to him that he cannot dislocate his arm without combining rotation and abduction. He may abduct the arm as much as he is able to do so in internal rotation in the coronal plane with impunity. These cases are usually in young men, and as has been said before, in athletes or in epileptics. Athletes may avoid dislocation by giving up those forms of athletics which tend to produce it. I have known two young men, who were my personal friends, both of whom were subject to this annoying difficulty. Both patients eventually outgrew it or changed their habits so that it did not occur. One of them, for instance, had to give up boxing because the arm would at times dislocate if he gave a forward blow. In doing this, the relation of scapula and humerus are practically the same as when they are in the pivotal position. He was a skillful athlete at other forms of amusement. It seems to me that for this type of patient it is better to change habits than to submit to operation.
In the cases of epileptics, it is imperative that the patient should wear an apparatus which prevents the combination of external rotation and abduction or should be operated upon. It has not been my fortune to have the care of any such cases. Should I be compelled to operate for this condition, I should at present choose the operation of Nicola. I here reprint some remarks made by Dr. Nicola at the discussion of Dr. Fowler's paper.
"For three years I have been using my own operation, which does not utilize any foreign material. It is done through one incision, the convalescence is short, and so far as I know there have been no recurrences on operations done by me as well as by about thirty other operators. It seems to me that it is getting more and more difficult for the student of orthopedics to decide which type of operation to use. In the end the operation that will become most popular is the one that is very simple to perform and can be done most frequently on almost any type of dislocation, no matter what the pathologic changes are (bony defects, muscle tears or capsular tears) ; and, finally, it is a matter of convalescence. In the operation which I have been doing, the line of incision begins just above the coracoid process and extends down and out in the line of the fibers of the deltoid. In my original description I stated that this should come between the pectoralis major and the deltoid, but I find that it is easy to approach it merely by going through the lines of the fibers of the deltoid. Before cutting the tendon, one should be sure to put transfixion sutures in both ends because frequently the arm may extend and the lower segment of the biceps tendon will slip behind the pectoralis and cause great anxiety. After the tendon is divided, a hole is drilled through the head of the humerus. I usually go anywhere along the bicipital groove and point the drill so that it comes out at the upper end of the angle of the head. The tendon is passed through the head and is sutured on itself, so that there is no muscle loss and the tendon has a tendency to restrict the movement and, therefore, keeps the head in the glenoid cavity. Some of the men have used this operation for fracture of the surgical neclc of the humerus when there has been downward displacement of the head into the axilla, and there they replace the head in position and drill a hole so that they maintain the head in position."
This operation appeals to me as more likely to fulfill the conditions required than any of the others. Fowler's operation also seems to me a rational procedure, but not so simple as Nicola's.
Extract from a personal letter from Dr. Nicola, June 6, 1930: "The cases reported in the reprint which you received, together with the rest, have been followed over a period of two years. The boxer has been back in the ring and has won two semifinal contests with no recurrence of dislocation. Case No. 3, which was an epileptic, was killed in an auto accident eight months after the operation. Through friendship with the coroner, I was able to examine the tendon of the long head of the biceps with special reference to the point which you made in your letter. I found that instead of thinning out of the long head of the biceps which extended to the glenoid cavity, the tendon above the humerus was thickened about the size of the little finger."
Extract from personal letter from Dr. Nicola, June 6, 1932: "I have personally done twenty-four of these operations with one hundred per cent cures. I have not heard of any recurrences from the various men who are associated with me at the Hospital for the Ruptured and Crippled. I hope that you will soon find an opportunity to operate upon such a case and to convince yourself that this operation is very simple to perform. I am now doing it through a two and one-half inch incision taken just below the clavicle on the inner side of the coracoid process and extending downward through the fibers of the deltoid muscle. The hole through the head of the humerus is made with a one-fourth inch gauge, instead of a drill. This facilitates matters considerably."
This operation I am sure could be readily done through my routine bursal incision which separates the deltoid fibers directly over the bicipital groove.
INFANTILE DISLOCATION OF THE SHOULDER
Lesions of the bursa or of the supraspinatus tendon in childhood apparently do not occur, at least they have never fallen within my experience. However, a not very infrequent lesion in childhood, namely, birth palsy complicated by dislocation of the shoulder, sometimes causes confusion in the diagnosis of shoulder lesions in later years. We see the shoulder deformed from a lesion which occurred at or soon after birth.
There has been much discussion as to whether the term congenital dislocation of the shoulder joint should ever be used. It seems very probable that a large number of so-called congenital subluxations, if not a majority of the published cases, were instances of obstetric palsy in which the dislocation remained after the paralysis had recovered. Infantile dislocation may be discussed under three headings, according to whether it existed before birth, occurred at birth or resulted soon after from paralysis caused at birth.
(1) Abnormality of development—true congenital dislocation. The existence of such a clinical entity has been questioned, but it has been established without any doubt, although it must be very rare. R. W. Smith of Dublin, in 1839, was the first to bring this condition before the profession. He published an account of three cases in the Dublin Journal of that year. Two of these were males, age 20. The dislocation was subcoracoid. The muscles about the shoulder were wasted. One patient had club foot. The third case was an insane woman, age 29, in whom the condition was bilateral.
At post-mortem examination there were facets just under the cora-coid, with a displacement of the capsule anteriorly to enclose the joint. The head of the humerus was flattened, and the acromion and coracoid elongated and hooked downward. In all the cases abduction was limited. Eleven years later Smith published two additional cases. In 1841 Guerin presented two cases and demonstrated a symmelian foetus which showed this abnormality on both sides. Since these reports, numerous cases have appeared in the literature. Grieg analyzed the cases of fifty-eight authors in the Edinburgh Medical Journal of 1923. He makes the following statement. "So far I have only found twelve cases reported to date in which evidence brought before the profession fails to justify any other conclusion than that they are cases of true primary congenital dislocation of the shoulder."
(2) Dislocation produced by obstetric manipulation or during birth. This group is open to criticism because proof of its existence is not satisfactory. T. T. Thomas was firmly of the opinion that traumatic dislocation not only occurs, but is the primary factor with regard to paralysis. He believed that paralysis is secondary to a rent in the capsule due to a traumatic dislocation. Taylor, writing in 1921, states that neither he nor any of three obstetricians of a large Lying-in Hospital had ever seen a case of Erb's palsy in which the subluxation preceded paralysis. In 1866 Loignan wrote a thesis for a Paris doctorate on the subject. He found that he could not dislocate the shoulder by manipulation. The constant lesion which occurred, if sufficient force were used, was a fracture of the humeral shaft through the soft bone under the epiphysis. Other investigators, notably Sever, have been unable to produce traumatic dislocation or rupture of the capsule by manipulation in infant cadavers. The writer feels that dislocation occurring at birth is so rare as to be negligible in diagnosis.
(3) Acquired subluxation due to injury of the plexus. Obstetric paralysis was first described by Smellie in 1768. He thought the condition was due to prolonged pressure on the arm while the child was in the pelvis. It was brought before the profession, however, by Duchenne, who in 1872 described four cases in infants and believed it to be due to pressure on the nerve trunks. Erb described the palsy in adults in 1874. Since that time it has been known as Erb-Duchenne paralysis. Erb believed it to be due to pressure on the fifth cervical root, known as Erb's point. Fieux opposed this view and adopted the theory that traction is responsible. He demonstrated on infant cadavers the fact that when the head is forcibly drawn away from the shoulder, the fifth cervical root is torn just proximal to its junction with the sixth nerve. With more force, the latter nerve may also be torn. Only the muscles of the upper arm are paralyzed. The palsy is usually flaccid.
Infants with Erb's palsy present a typical history and appearance. There is usually a difficult birth where traction on the head has been made under ether relaxation. The arm hangs limp and vertically at the side, the elbow is extended and the forearm pro-nated. There is inability to abduct, elevate, outwardly rotate, or supinate. There is extreme internal rotation so that the palm often faces outward. After a short time, there is wasting from disuse, and flattening of the shoulder soon appears. Passive motions' are free at first, but the healthy muscles soon contract and produce limitation of motion—notably of external rotation. The muscles paralyzed are the deltoid, supra- and infra-spinatus, teres minor, biceps, brachialis and brachioradialis. There is no sensory disturbance.
Clark, Taylor and Prout estimated one case of palsy in 2,000 births. Most cases of birth palsy show some luxation of the head of the humerus. Fairbanks saw twenty-eight subluxations in thirty-seven cases of palsy, or seventy-six per cent; Thomas reported nine in twelve. Taylor has reported sixty-eight cases, forty-six of which showed subluxation. He has never seen the condition in patients less than six weeks old. Of those patients who had palsy, who were more than six weeks old, seventy-seven per cent showed subluxation. In 109 X-ray studies reported by Sever in 1916, sixty-four or fifty-nine per cent showed subluxation. The ages in this series varied from one day to eighteen years.
It should be noted that this form of dislocation is posterior, while the first two forms are anterior or inferior.
Mechanism of Posterior Subluxation. The appearance of the arm soon undergoes a change from the flaccid condition which follows the immediate injury for a few weeks after birth. The upper arm is brought forward and adducted by contraction of the well muscles. The elbow is usually a little flexed, the pronated forearm passing downward and inward across the front of the body. Abduction is checked before the arm comes to a right angle. Backward motion is usually impossible and external rotation is markedly limited. With the elbow at the side, it is often impossible to rotate the humerus out sufficiently to bring the forearm into the forward plane. The bones of the affected side—the humerus, scapula and clavicle—are smaller than those on the opposite side. This is an important point in the diagnosis of late cases. The front of the shoulder is flattened, while there is a fullness behind, below the acromion, due to the head of the humerus. The muscles which tend to prevent posterior dislocation are the teres minor, supraspinatus, infraspinatus, and posterior part of the deltoid. The pectoralis major, the teres major and latissimus dorsi are rarely even partially paralyzed and rotate the humerus strongly inward. The subscapularis acts as a powerful internal rotator. These muscles become contracted while the paralyzed ones are stretched. The teres major and latissimus dorsi exert traction downward and posteriorly. The anterior portion of the capsule becomes shortened secondarily. Since the arm is held in an internally rotated position, there is a constant jstrain on the neck of the humerus, tending to twist it backward. In the plastic young bone, this twisting occurs and the plane of the head of the bone to the shaft may be changed ten or fifteen degrees. The dislocation is not truly posterior—it is rather a rotation of the head than a dislocation, so that the articular portion is rotated backward and the side of the head lies on the glenoid without having escaped from its capsule.
During the first year nothing can be seen in the way of bony deformity in the X-ray, except possibly a slight posterior subluxation and relatively small size of the head compared to that of the other side. As the child grows older, the subluxation increases. There is increased outward displacement and elevation of the scapula. The acromion and coracoid become hooked downward in front of the head of the humerus. The clavicle is shortened and its curves are more marked than in the normal. The coracoid process is usually elongated. The glenoid becomes shallow. These changes of the bones occur while the paralysis exists, and even if the paralysis clears up, they persist.
Treatment. In early cases the arm may be held in abduction, elevation, external rotation and supination by a light wire splint. Sever, however, prefers to let the child use the hand and arm freely with the risk of contractures. Passive motion and massage are carried out at frequent intervals. Operation is deferred until the child is three or four years of age. Once contractures have developed, it is best to cut the contracted muscles. Manipulation is of little value because of the tendency to recurrence, unless the paralyzed muscles have regained their tone. Sever has described his operation at length in a paper read before the Section on Orthopedic Surgery of the American Medical Association, 1925. He cuts the pectoralis and subscapularis tendons and removes one-half inch to three-quarters inch of the tip of the coracoid with its muscle attachments. If necessary he removes the hooked acromion to allow reduction. The arm is put up in a light splint in abduction, elevation, external rotation and supination. Muscle reeducation by active and passive motion is begun after eight to ten days. The splint is worn night and day for three months, but is removed daily for exercises.
Prognosis. This depends largely on the recovery of the paralyzed muscles in early cases. If the child is seen early, contractures and subluxation may be minimized by passive motion until the nerves have regenerated. In late cases, however, where contractures have developed and there is no tendency of the nerves to regenerate, operation has to be resorted to and gives a good, hut not brilliant, functional result. Sever records partial recovery in 297 of 394 cases which were operated upon. After operation there is great difficulty in inwardly rotating the arm. He states that this may be eventually overcome, however.
I have had very little personal experience in these cases, but the following case taught me such an important lesson that an account of it is presented in the hope that it may stimulate some one to follow up a series of such cases in which operations had been done in childhood.
CASE 70.
A strong boy, age 14, was referred to me for trouble with his shoulder, with the story that he had had difficulty since he was a baby, and that while he was a very strong, active boy otherwise, he was greatly handicapped by his shrunken, weak, deformed right arm. The diagnosis in the case puzzled me a good deal at first, for there was no paralysis, and the X-ray simply showed a rather small and deformed humeral head and glenoid cavity. In spite of this, by palpation, it was easy to feel that the head of the humerus was posterior to the glenoid under the acromion. Both the coracoid and the acromion were hooked down in an unnatural manner, which was easy to understand when one recognized the true character of the lesion, for the acromion process had nothing beneath it and was not performing its normal function. All parts of the shoulder, including the bones, were smaller than those of the opposite side. There was practically no motion in the scapulo-humeral joint and the arm was held in internal rotation. An extraordinary amount of compensatory mobility had developed in the motion of the scapula on the chest wall— not only in flexion and extension, but in abduction and adduction.
It was clearly a case of birth palsy in which the bones had remained out of place after the muscular paralyses had recovered, and therefore the patient now only suffered from the consequence of the luxation.
I operated on June 16, 1921, through a "sabre-cut" incision, and to my surprise, found that the cartilaginous surfaces of the glenoid and of the head of the humerus had remained in nearly a normal condition, although they had been separated for so many years. The capsule was stretched and distorted, but not disrupted. The cartilaginous surface of the glenoid was rather puckered and the articular head of the humerus was small and rather misshapen, although less so than one would think from the appearance in the X-ray, which of course showed the surface of the bony centers of the epiphysis and not the cartilage. The contraction of the subscapularis and pectoralis major was so great that I had to divide their tendons in order to get the head of the bone in place. The coracoid process was so deformed that I had to excise about two-thirds of it subperiosteal^ in order to reduce the humerus. The "sabre-cut" incision, of course, mobilized the acromion. After reducing the head of the bone, I was able to put four silk sutures "a-distance" to reunite the cut ends of the subscapularis. I did not attempt to correct the torsion of the neck, although it caused some eversion of the arm when the head of the bone was in place. The whole wound was sutured, and the patient was put up in plaster in semi-abduction and semi-external rotation.
It was most remarkable to watch the boy's convalescence. There was a good surgical recovery, but the miraculous part was to see the promptness with which the bones and muscles tended to grow into normal condition. Within six months he had nearly normal use of his shoulder, and the condition of the muscles had greatly improved.
As the patient lived in another city I lost track of him about six months after the operation and did not see him again for ten years, when I looked him up in preparation for this book. It is fortunate that I did so, for the lesson which I learned was important and may be of help to others.
During the ten years that had passed, the boy had become a man of twenty-four, whose occupation was in moving buildings. He did much of the manual labor himself. When he came into my office he looked strong and vigorous, and I had to ask him which shoulder was the bad one. Then my disappointment came.
A skillfully made movable pad inside his coat concealed the small size of his right shoulder. His vigorous handshake and well-developed forearm gave no hint of the practically ankylosed joint which was displayed when he removed his clothes. On closer examination I found both coracoid and acromion clutching down on the head of the bone like crooked fingers grasping it and holding it fixed. It appeared as if the acromion process had bent downward from the point where I had divided it and had become fixed in this position.
After a time the explanation occurred to me. At fourteen, the acromion and coracoid are cartilaginous epiphyses, for they have not yet ossified. After my operation, although the head of the humerus was in place, it was small and underdeveloped because of imperfect function for fourteen years. Consequently the cartilaginous acromion and coracoid became bent down over it, grasped it, and then, at about twenty, turned to bone and held it fixed. I did not at the time of the operation realize that the greater part of the acromion does not unite with the spinous process until about twenty. I think now that if I had insisted that this boy should have slept with his arm elevated until he was twenty, and had kept up appropriate exercises, he might have obtained a more perfect shoulder. It is not a great hardship to form the habit of sleeping with the arm in the hammock position. Many people do this by preference. He had been able to hold his arm in this position when I last saw him six months after the operation. Later the strength of the divided internal rotators returned and tended to rotate the arm to its old position, and also to resist elevation in external rotation. The head of the bone being small, the cartilaginous acromion slowly yielded to fit over its convexity. I think that it is highly probable that if the late results of other operations which have been done for these cases were critically examined, the same disappointing condition might be found in later years. Operations should not be undertaken on these cases unless the parents are warned that the patient should be under the surgeon's care until his epiphyses are united; i.e., when the patient is about twenty. I am inclined to think that nature's results at the end of ten years would compare very favorably with those of surgeons.
ACROMIO-CLAVICULAR DISLOCATION
A brief consideration of lesions of the acromio-clavicular joint seems advisable, although strictly speaking, neither the subacromial bursa nor the supraspinatus tendon are involved. One must remember that the coraco-acromial ligament intervenes between these structures. When this joint is dislocated the coraco-acromial ligament goes intact with the scapula. In severe cases the coraco-clavicular ligaments (conoid and trapezoid) are torn.
Mechanism. The acromio-clavicular joint, itself, is weak, but the conjunction of the two bones derives its strength from the conoid and trapezoid ligaments which are attached to the coracoid process of the scapula. Upward dislocation of the clavicle is favored by the upward and outward slope of the joint. The clavicular facet looks downward, outward, and backward. Dislocation is almost always caused by direct violence. A blow on the back of the acromion or a fall on the tip of the shoulder drives the acromion downward, inward, and forward, and the clavicle with the coracoid process as a fulcrum is torn away.
Dislocation is classed as complete or incomplete according to whether or not the facets clear each other. The ligaments of the joint itself are more or less torn, even in incomplete dislocation, but the conoid and trapezoid ligaments are usually torn in complete dislocation.
Diagnosis. The diagnosis is to be made from the history of trauma, pain and disability. The outer end of the clavicle is prominent and movable, and can be readily reduced, but reduction is hard to maintain if the coraco-clavicular ligaments are ruptured.
Treatment. Upward, outward, and backward traction on the scapula is indicated and can be applied by various braces or by recumbency. The most favored method is the clavicular cross. A T-shaped splint is applied to the back, and the shoulders strapped to the cross arms.
Open reduction and fixation are occasionally necessary. Several operations have been devised, most of them using fascial strips. Representative among these may be cited Bunnell's ingenious method. He threads a cord of fascia through holes in the acromion and clavicle, and places a loop under the coracoid process.
Prognosis. If the reduction can be maintained, the chances are good that a patient will regain function in the course of several months, but soreness and some pain may persist for years. Arthritic changes may take place. I personally have never found it necessary to operate on acromio-clavicular dislocation, but in extreme cases I should recommend Bunnell's operation.
ACROMIO-CLAVICULAR ARTHRITIS
In contrast to the mechanism of the scapulo-humeral articulation, that of the acromio-clavicular joint is typical of the kind in which arthritis is prone to occur. It is a hinge joint with a very limited degree of motion. For its size, when in action, it carries an immense burden of weight. For instance, as one pushes open a heavy door, this little joint has to bear the equivalent weight of almost the^ whole power exerted. The same is true of the joint on the sternal end of the clavicle, but that joint has a much larger surface area. In laboring men who carry or lift heavy burdens, spurring from arthritis of the acromio-clavicular joint is so common as to form almost as normal a tissue as the great calluses in their hands. In many of the older individuals, the rims of new-formed bone actually fuse, so that the joint becomes obliterated. These changes may progress with very little pain and discomfort to the individual, or they may be accompanied by the usual signs of arthritis, which occasionally are so severe that they incapacitate the patient.
The acromio-clavicular joint holds an exposed position on the shoulder, and falling objects not infrequently strike the joint directly—perhaps breaking some of the small bony lips, causing hemorrhage about or in the joint. Such cases may be laid up for months on account of the local tenderness when they attempt to use the arm. I find it very difficult, in giving an opinion on compensation cases, to state when such individuals should be expected to return to work. The X-ray appearance is far from being a criterion. A man may have a very ragged and hypertrophied-looking joint and yet be conscious of no symptoms. Another man with barely perceptible changes may have much local tenderness. On the whole, it is surprising how well these laboring men are able to bear acromioclavicular arthritis. The diagnosis of these lesions rests entirely on the readily ascertained facts of localized swelling and tenderness, supported by the X-ray evidence of lipping of the joint. Confusion in diagnosis only arises when one allows one's self to center his attention on this joint and to ignore other really more important lesions. Never forget that this condition may attract your attention too readily, and by its presence conceal a lesion of the supraspinatus which is far more serious. Acromio-clavicular arthritis must be judged by the degree of symptoms, not by its X-ray appearance, for often there is much lipping of the edges of these joints and yet no symptoms at all.
Treatment. As a rule, these cases respond well to rest. A few weeks' confinement of the arm in a sling soon after a bruise on one of these joints is all that should be attempted. I am convinced that complete fixation of this joint is unfortunate. I do think that rest is very important in acute stages. Patients who have had prolonged symptoms have usually had either prolonged energetic treatment or prolonged fixation.
In a few subacute and prolonged cases, I have cut into the joint with the same idea that one has in cases of periostitis, where one incises to cause relief of tension. As a rule, however, I believe that simple rest is the only form of treatment which is important. The usual physiotherapy methods may be of some use, but my personal experience with them has been little.
Remember that the acromio-clavicular joint is not in immediate anatomic relation with the subacromial bursa. The coraco-acromial ligament intervenes. Therefore, acromio-clavicular arthritis does not prevent rotation or abduction in the scapulo-humeral joint, except in extreme positions. If these motions are not present, do not blame the acromio-clavicular joint entirely, even if it is swollen and tender.
Arthritic changes in this joint commonly occur after luxation or subluxation, and soreness may continue many months and sometimes a few years after such accidents. Men who do their own work generally continue at it in spite of this protracted soreness, but employees are apt to find their shoulders too sore to permit labor, if their compensation is paid. Thus this little lesion may be the cause of their never working again, for it is a commonplace that a year of loafing is a serious matter for an elderly laborer. Surgical obliteration of the joint should be considered, in some cases at least, as a mental stimulant. It is not an important joint.
BIBLIOGRAPHY
BANKART, A. S. B. Recurrent or habitual dislocation of the shoulder joint.
Brit. M. J. 1923. 2. 1182-1133. BUNNELL, S. Fascial graft for dislocation of acromio-clavicular joint.
Surg. Gyn. and Obst. 1928. 46. 563-564. CARRELL, W. B. Habitual dislocation of the shoulder.
J. A. M. A. 1927. 89. 948-952. DELBET, P. Des luxations anciennes et irreductibles de l'epaule.
Arch. Gen. de Med. 1893. ser. 7. vol. 81. 19-39. DOLI.INGER, J. Die Veralteten traumatischen Verrenkungen der Schulter; des
Ellenbogens und der Hufte.
Ergebnisse der Chir. und Orthop. 1911. 3. 83-194. DOI.LINGER, J. Das anatomische Hinderniss der Reposition bei veralteten sub-
coracoidealen Schulterverrenkungen und meine Methode zur blutigen Reposition dieser Verrenkung.
Deut. Zeit. fur Chir. 1902-03. 66. 819-335. DUCHENNE, G. B. Physiologie des mouvements.
Paris. J.-B. Bailliere et Fils. 1867. pp. 7-17. EDEN, R. T. Habitual dislocation of shoulder.
Zentralbl. f. Chir. 1920. 47. 1002. ELIASON, E. T. Nelson's System of Surg. vol. 3. p. 292-293. FIEUX, see Bibl., Chap. XI. FINSTERER, H. Zur Frage nach der zweckmassigsten Behandlung der habituellen
Schulter luxation.
Wien. Med. Woch. 1924. 74. 1232-1237. FOURMESTRAUX, J. DE. Les luxations recidivantes de l'epaule; pathogenie; traite-
ment.
Arch. Med.-Chir. de Province. 1920. 10. 18-26. FOWLER, E. B. A new operation for recurrent dislocation of the shoulder.
J. A. M. A. 1932. 98. 476-478. GERSTER, A. G. Subcoracoid dislocation of the humerus; paralysis of the serratus
magnus; arthrotomy.
Med. News, Phila. 1884. 44. 423. GOEBEL, W. Zur Prognose der traumatischen Schultergelenksluxation.
Zeit. fur Artzl. Fortbildung. 1909. 6. 347-855. GRASSNER, R. Die Briiche des grossen Oberarmhockers.
Veroff. aus dem Gebiete des Milit.-Sanitat. 1906. 85. 180-198. GRATZ AND ROBINSON. Am. J. Surg. XV. 1932. 71. January. GUBLER, H. Zur Prognose der Schultergelenksluxationem.
Schweiz. Med. Woch. 1922. 52. 960-964.
Abst. J. A. M. A. 1922. 79. 1964. HENDERSON, M. S. "Tenosuspension" for habitual dislocation of the shoulder.
Surg. Gyn. and Obst. 1926. 43. 18-25. HILDEBRAND. Zur operativen Behandlung der habituellen Schulterluxation.
Arch, fur Klin. Chir. 1902. 66. 360-364.
KELLER, W. L. Treatment of chronic recurrent dislocation of the shoulder by
crucial capsular plication.
Ann. Surg. 1925. 81. 143-148. KOCHER, THEODORE. Eine neue Reductionsmethode fiir Schulterverrenkung.
Berl. Klin. Wchnschr. 1870. 7. 101-105.
Bull. Soc. Med. de la Suisse Rom. Lausanne. 1873. 7. 819-330. 3 pi. KUTTNER. Zur Prognose der traumatischen Luxation.
Zentralbl. fur Chir. 1908. 35. Beilage p. 155-157. LANDES, T. L. Recurring dislocation of the shoulder joint.
Brit. Med. J. 1921. 2. 321-822.
LEXER, K. Nachuntersuchungen von traumatischern Schultergelenksluxation. Beitr. zur Klin. Chir. 1910. 70. 221-235.
LOEFFLER, F. Die Behandlung der habituellen Schulterluxation durch Bildung
eines extraartikularen Hemmungsbandes.
Zbl. fur Chir. 1920. 47. 324-326. MANDL, F. Bemerkungen zur Operation der habituellen Schulterluxation.
Deut. Zeitschr. fur Chir. 1925. 191. 108-120. NICOLA, T. Recurrent anterior dislocation of the shoulder; a new operation.
J. Bone and Joint Surg. 1929. 11. 128-182.
NICOLA, T. Recurrent dislocation of the shoulder; its treatment by transplantation of the long head of the biceps. Amer. J. Surg. 1929. 6. 815.
NICOLA, T. Operation for relief of recurrent dislocation with presentation of
patients.
Amer. J. Surg. 1931. 11. 119-121. OUDARD. La luxation recidivante de F6paule (varied ante>o-interne).
J. de Chir. 1924. 23. 13-25.
Abst. J. A. M. A. 1924. 82. 1004. OUDAFD. La luxation recidivante de l'6paule (variete ante>o-interne).
Presse Med. 1928. 86. 201-202. PERKINS, G. Discussion on the painful shoulder.
Proc. Roy. Soc. Med. (Sect. Orthop.) 1929. 22. 20-80. PERTHES. Munch. Med. Woch. 1905. H, 10. s. 481. PERTHES, G. Results of surgerv in habitual dislocation of humerus.
Dtsch. Ztschr. f. Chir. 192*5. 194. 1-24. Also J. A. M. A. 1926. 86. 589.
PILZ, W. Zur RHntgenuntersuchung der habituellen Schulterverrenkung. Arch, fur Klin. Chir. 1925. 135. 1-22. Abst. J. A. M. A. 1925. 85. 75. Also Zbl. Chir. Soc. 22, s. 1390. 1928.
PLUMMER, W. W. & POTTS, F. N. Two cases of recurrent anterior dislocation of the shoulder. J. Bone and Joint Surg. 1925. 7. 190-198.
PRESTON, M. E. Fractures and dislocations. C. V. Mosby Co., St. Louis. 1915. p. 11-108.
RIVIERE, G. Capsulorrhapie de l'articulation de l'£paule pour luxation recidivante. Lvon Chir. 1918. 15. 437-439. Abst. J. A. M. A. 1919. 72. 612.
SCHI.AEPFER, K. Uncomplicated dislocations of the shoulder; their rational treatment and late results. Amer. J. Med. Sc. 1924. 167. 244-255.
SELIO, R. Die bei der habituellen Schulterluxation gebrauchlichen Operations methoden von anatomischen Grundsatzen aus betrachtet. Was leistet der Musculus supraspinatus. Deut. Zeit. fur Chir. 1915. 132. 581-588.
SEVER, J. W. The rational treatment of fractures of the upper end of the humerus. Report of end results. J. A. M. A. 1923. 80. 1603-1608.
SEVER, J. W. Recurrent dislocation of the shoulder joint. Mechanical consideration of its treatment. J. A. M. A. 1921. 925-927.
SINZ, P. Inaugural-Dissertation. Erlangen. 1982.
SPEED, K. Recurrent anterior dislocation at the shoulder. Operative cure by bone graft. Surg. Gyn. and Obst. 1927. 44. 468-477.
SPEED, K. Fractures and dislocations.
Lea and Febiger, Phila. 1916. p. 857-440.
SPITZY, H. Stabilization of the shoulder joint for habitual dislocation.
Surg. Gyn. and Obst. 1928. 46. 256-257. STEVENS, J. H. The action of the short rotators on the normal abduction of the
arm, with a consideration of their action in some cases of subacromial bursitis
and allied conditions.
Amer. J. Med. Sc. 1909. 138. 870-884. STEVENS, J. H. Dislocation of the shoulder.
Ann. Surg. 1926. 83. 84-103. STEVENS, J. H. Fractures of the upper end of the humerus.
Ann. Surg. 1919. 69. 147-160. STIMSON, L. A. Fractures and dislocations.
Lea and Febiger, Phila. 1917. TAYLOR, R. T. Fracture dislocation of the shoulder. Arch. Surg. 1928. 17. 475-483. THOMAS, T. T. Habitual or recurrent dislocation of the shoulder. Etiology and
pathology.
Amer. J. Med. Sc. 1909. 137. 229-246.
J. A. M. A. 85. No. 16, s. 1202. 1925. TREVES, F. Surgical applied anatomy.
Lea and Febiger, Phila. 5th ed. VALTANCOLI, G. Sulla lussazione abituale di spalla.
Chir. d. Organi di Movimento. 1924. 9. 131-140. WARREN, J. C. Am. J. Med. Sci. 1846. XI. WILSON, P. D. & COCHRANE, W. A. Fractures and dislocations.
Lippincott & Co. 1925. p. 59-153.
NOTE—Sinz (1932) gives a very extensive Bibliography. He recommends a bone transplant to the glenoid (after Perthes or Eden) but apparently was unaware of the work of Nicola.
